The
use of and diet, habits and supplements to help prevent medical
problems.
Part
III: Diet Choices, Healthy Habits and Supplements
Every
one desires to live long, but no one would be old.
-
Jonathan Swift (1667-1745), Thoughts on Various Subjects, Moral and
Diverting 1
To
lengthen thy life, lessen thy meals.
-
Benjamin Franklin, Poor Richard's Almanack, June 1733 2
Calories
are a primary cause of aging, and the limiting factor
in lifespan.
Key
insight: cutting calories slows the aging process and prolongs life.
Aging
is due to a combination of years of age and total calories eaten in
your lifetime3;
The
road to aging is paved with calories.
The
simplest way to reduce calories is to reduce portion size: use a
small plate!
By
my calculations, every calorie above the absolute minimum ages
your body and your mind and hastens death by about 31 seconds
(+/- 10). This means that you age one day (and lose one
day of life span) for every 2800 calories you eat - above a
starvation diet with good nutrition (adequate protein, fats, vitamins
and minerals). Carrying an extra pound of weight for one year costs 2
days of life span. In dollar terms, a candy bar might cost $20 in
potential lost wages. (See “Effect
of CR.XLS” for calculation details). A 40-year-old man can
live 8 years longer by eating 25% less; a 15-year-old can live 16
years longer by eating 25% less. Slowing aging means MORE YOUTH, not
more old age.
Turn
this around: it is VERY expensive – in terms of money, aging,
disability and early death – to keep your weight up!
Can
you afford to stay plump?
Last
updated 2007-01-17
NOTE:
This document is very long. I have not revised it thoroughly. Much in
the last half of the document is outdated. I think that no
supplement, food, or habit - by itself or in combination with others
- will be as effective as moderate caloric restriction (CR, to a BMI
of about 18.5).
Table:
Personal goals, many not yet achieved
These
parameters are directly affected by lifestyle choices (diet, CR,
exercise, supplements, etc.), and have substantial effects on
lifespan, quality of life, and risk of serious disease.
|
Parameter
|
Goal
|
Current
|
Date
|
|
BMI
(Weight)4
|
17
(115 lbs)
|
20
(138 lbs)
|
2006-07-15
|
|
Blood
pressure5
|
<
115/75
|
114/66
|
2006-05-11
|
|
LDL
cholesterol6
|
<
80
|
83
|
2006-05-05
|
|
HDL
cholesterol7
|
>
50
|
70
|
2006-05-05
|
|
HbA1c8
|
<
5.0
|
5.5
|
2001-10-01
|
|
Fasting
glucose9
|
<
90 or < 81
|
88
|
2006-05-05
|
|
Fasting
triglyceride9
|
<
150
|
58
|
2006-05-05
|
Table
1: Interventions
This
table summarizes what I think are the most important interventions,
in order of importance to health. Rating is my own assessment
of the intervention, based on its importance and my confidence
in the scientific backing to support it (1 = very important with
strong suggestive evidence; 5 = possibly helpful, with some evidence
to support it).
|
Rating
|
Intervention
|
What
I do or think should be done
|
|
1
|
Caloric
restriction with optimal nutrition (abbreviated CR or CRON)
Note
well: this is approximately twice as important as everything else
put together!
|
Goal
body mass index approximately 17, by reducing calories, not just
by exercise.
N.b.,
Exercise is very good, but exercising without dieting is
not the best way to live longer or slow the aging process.
|
|
1
|
Modify
fat intake, including increasing Omega-3 fat & monounsaturated
fats (MUFAs)
|
Caloric
restriction
Completely
avoid partially hydrogenated oils (trans fats)
Avoid
saturated fats, avoid most animal fat
Eat
moderate amounts of: tree nuts (unsalted & raw), wild
salmon, freshly ground flaxseed, extra virgin olive oil, avocado
Cook
with olive oil, preferably extra virgin
|
|
1
|
Reduce
cholesterol and triglyceride levels
|
Caloric
restriction
Avoid
trans-saturated fats, animal fat
Eat
flax meal, fruits & vegetables, tree nuts, high-fiber
foods, orange peel
Avoid
most carbs (rice, plain bread, sugar, potatoes, pasta, foods made
largely of white flour, etc.)
Consider
statin drugs (only if cholesterol is too high and other
things fail)
|
|
1
|
Keep
blood pressure low (less than 115/75)
|
Caloric
restriction
Low
salt intake, exercise daily, use potassium chloride (instead
of salt, or 50/50 with salt if needed), limit alcohol intake, high
folic acid (4 mg/day), take 6 mg of melatonin each night, eat a
high protein diet (mostly vegetable-based), soluble fiber,
magnesium
|
|
1
|
Take
safety precautions
|
Drive
safely, use seat belts, drive in a safe car with air bags,
fire safety, follow government hazard preparation recommendations,
hip protectors for the elderly
|
|
1
|
Take
certain supplements
|
Vitamins
D, B12, folate (about 4 mg / day vs. HTN), magnesium,
benfotiamine, green tea extract, melatonin, glucosamine &
chondroitin
A
little zinc & selenium; iron if really needed
Avoid
vitamin E supplements (alpha tocopherol)
Possibly:
R(+) ALA
|
|
1
|
Exercise
daily
|
Run
1 mile each day, do calisthenics and stretching.
|
|
2
|
Reduction
of homocysteine (a major risk factor for heart disease &
Alzheimer’s)
|
Caloric
restriction
Eat
a low-methionine diet: this can be done by getting protein from
vegetables instead of animals (milk, eggs or meat)
Take
supplemental vitamins: folate & B12
|
|
2
|
Reduce
glycation (damages proteins & hardens arteries)
|
Caloric
restriction
Reduce or eliminate “useless” carbohydrates,
cook meat at low temperatures, reduce mixing sugar and protein in
cooked foods, benfotiamine
Possibly:
R(+) ALA
|
|
2
|
Avoid
sun damage
|
Clothes,
zinc oxide- or titanium dioxide- based sun block, hat,
UV-protection sunglasses, eat orange peel
But,
be sure to take 800 units/day of supplemental vitamin D in the
form of D3
Caloric
restriction (Perhaps - it reduces the area exposed to
the sun)
|
|
2
|
Reduce
inflammation
|
Caloric
restriction
Floss
& brush teeth, treat infections and skin problems
If
you have risk factors for heart attack (especially older men),
take a baby aspirin each day or every other day
|
|
2
|
Vaccinations
– keep up to date
|
Influenza
shot yearly, Pneumovax, hepatitis B, chickenpox / shingles,
tetanus, etc. In short, take all that are recommended
|
|
2
|
Eat
a high-fiber diet
|
Fruit
& vegetables; bran (insoluble fiber), whole grains, freshly
ground flax seed
Soluble
fibers: glucomannan, psyllium, methylcellulose and guar (these are
concentrated sources of soluble fiber, shown to lower cholesterol
levels by 10%)
|
|
2
|
Medical
tests periodically
|
Blood
pressure, CBC, HbA1C, colonoscopy (starting at age 50), PSA,
cholesterol (HDL & LDL) & lipids, CRP, eye exam for
glaucoma, breast & pelvic exams for women
|
|
2
|
Greatly
reduce in diet
|
Food!
(i.e., caloric restriction)
Salt,
red meat (worst if grilled, charred or cooked at high
temperatures), omega-6 fat (corn, soy & cottonseed oils etc.),
cured meats, excess fluoride,
saturated and trans-saturated fats
Possibly:
soy, peanuts
|
|
2
|
Increase
the proportion of certain foods
|
Eat
a variety of tree nuts, berries, spinach, kale, sprouts, broccoli
& related veggies, tomato paste, coffee, green tea (only as
extract capsules), pomegranate juice, fruit
|
|
3
|
Reduce
iron load
|
Caloric
restriction (less total iron intake)
Give
blood if you are a man, avoid iron supplements, reduce or
eliminate red (mammal) meat
However,
take care to avoid iron deficiency
|
|
3
|
Avoid
certain cooking techniques
|
Charred
meat, over-cooking of fish or meat, high-temperature cooking of
most foods, cooking with polyunsaturated oils such as canola,
sunflower or flax oil, cooking sugars and meats together
|
|
4
|
Eat
more than the RDA of protein
|
From
vegetable sources such as broccoli, spinach, lentils, peas and
tree nuts (n.b., vegetables like broccoli & spinach have far
more protein per calorie than do beans and nuts)
|
|
5
|
Avoid
aluminum (possible cause of Alzheimer’s
disease)
|
Use
non-aluminum-based deodorants, minimize foods that use alum-based
baking powder (read the label), drink reverse-osmosis filtered
water, avoid certain foods with aluminum (some pickles), avoid
aluminum foil on foods, etc.
Possibly
avoid antacids such as Mylanta (most are made with aluminum)
|
Table
of Contents
Caloric
restriction – eating less – is the main and by far most effective
approach to improving health and prolonging life. Caloric restriction
keeps you younger longer. In addition, there are certain choices of
diet, habits and supplements to help prevent medical problems. All of
them are documented in the tables and text below, with references. In
brief:
Fats
Modify your intake of fats.
Increase certain fats:
- Omega-3 fat: freshly ground flaxseed, salmon and canola
- Monounsaturated fats: MUFAs, from tree nuts (not peanuts),
avocados, & olives
- Cook with olive oil
Fats should
comprise between 25-40% of your dietary calories.
Avoid
certain fats:
- Trans-saturated fats (this is five times as
bad for you as saturated fat!!): partially hydrogenated vegetable
oils
- Animal fats (especially mammalian): beef, pork,
mutton, butter, whole milk etc.
- Saturated fats: animal fat,
palm oil & coconut oil, fully hydrogenated vegetable oil, brazil
nuts
- Excessive omega-6 fats: corn oil, corn-fed beef &
pork, etc.
Exercise
daily, in moderation.
Vitamins,
minerals and supplements Take
supplements or enough dietary vitamins to reduce homocysteine (see
Homocysteine,
likely to be a major risk factor for heart disease, stroke &
Alzheimer disease) take a few supplemental vitamins: folate, B12, D.
Take
safety precautions: Drive safely, use seat belts, drive in cars with
air bags, and practice fire safety.
Hypertension
Keep blood pressure low (<115/75): very low
salt intake, take supplemental potassium
(substitute KCl (NuSalt) for some of the NaCl) & magnesium &
folate, exercise, alcohol intake limited (women: < 2/day;
men < 3/day), fruit and vegetables and low-fat dairy.
Vegetables
& fruits Eat certain fruits &
vegetables: a variety of nuts, legumes, tea (or tea extract capsules
– this is what I do), pomegranate, berries, spinach, kale,
sprouts, prunes, broccoli & the like, red pepper, tomato paste,
vitamin C, selenium (in nuts), purple grape juice, pomegranate
juice, turmeric (along with pepper), magnesium-rich foods (whole
grains, nuts, leafy green vegetables). Eat foods with soluble
fibers: flax, glucomannan, oat bran, psyllium and guar.
Avoid
sun
damage: Clothes, sun block, hat, and polycarbonate/UV-protection
sunglasses.
Eat
a “Mediterranean
diet”: olive oil, fish,
vegetables, fruit, and red wine.
Nuts
Cholesterol
and triglycerides
Meat
Methionine
restriction seems to have a large
positive effect on lifespan & prevention of diabetes. Animal
protein sources (e.g., beef, pork, fish, milk, cheese, and eggs)
have about twice as much methionine per gram of protein compared to
vegetable protein sources (broccoli, lentils, peas, spinach, etc.).
This may a reason that vegetarians are generally healthier than meat
eaters.
Protein
Carbohydrates,
glycemic index, and glycemic load
Advanced
Glycation Endproducts and cooking methods
Bran
and whole grains
Fiber
(psyllium, guar, glucomannan etc.)
Tea
and Coffee
Wine
and alcohol
Toxins
Summaries
of prevention measures for specific diseases
Brush
your teeth
Safety
measures
Genetics
Obviously, this is not something you can do anything about in
retrospect! However, identification of truly important factors might
eventually lead to medical interventions that mimic the effects of
the genes.
Caution
#1: Many human studies show benefit from one or another intervention,
such as eating vegetables, fish, or wine, etc. The inference that the
intervention caused the benefit is not necessarily true, even when
the study design is flawless (rare). Eating vegetables for example
could simply be a marker for those with genes to protect against
heart disease. The finding has to be supported by animal studies, a
reasonable pathophysiological mechanism, etc. Other studies show
benefit in animals, but have to be confirmed in humans. Thus, most of
the recommendations in this document are based on suggestive – NOT
CONCLUSIVE – data.
Caution
#2: Be cautious about inferring cause from effect. For example, when
people eat fruit and vegetables, there is a reduction in many
diseases. This may be due directly to the fruit and
vegetables, but it may be for other reasons, e.g. because these fruit
and vegetables substituted for other foods that are bad for you. The
suggestions in this document are particularly susceptible to this
problem.
Warnings
Avoid
Atkins’ diet (in the early popular form). In one form, this
diet promotes eating such things as animal fat, red meat, butter,
trans-fats (margarine and many prepared foods) etc. This does help
decrease your appetite and you may lose a small amount of weight, but
you run greatly increased risks of common, deadly and debilitating
diseases such as heart disease, hypertension, stroke, cancer,
Alzheimer disease and Parkinson disease. When you eat fatty foods (I
do), you should do so carefully: eat mono-unsaturated fats (MUFA)
found in nuts, olive oil, avocados etc. Also, specifically eat foods
with omega-3 fats, such as wild salmon and possibly freshly ground
flax seed. These fats are in fact GOOD for you and tend to prevent
some of the problems that Atkins causes.
Folks,
this
web site interview 10
is worth reading in detail, by all. Why? Well, consider how much
money and time you will spend on medical care for yourself, and then
consider this quote from Walter Willett, MD (that I KNOW is backed up
by outstanding data - I have reviewed this data myself): "The
potential impact of healthy diet, when you combine it with not
smoking and regular physical activity, is enormous. For example, our
studies have shown that we could prevent about 82 percent of heart
attacks, about 70 percent of strokes, over 90 percent of type 2
diabetes, and over 70 percent of colon cancer, with the right dietary
choices as part of a health lifestyle. The best drugs can reduce
heart attacks by about 20 or 30 percent, yet we put almost all of our
resources into promoting drugs rather than healthy lifestyle and
nutrition…Walter Willett is professor of epidemiology and nutrition
at Harvard School of Public Health, a professor of medicine at the
Harvard Medical School, and the author of Eat, Drink, and Be
Healthy: The Harvard Medical School Guide to Healthy Eating."
Some
of the supplements or diet modifications may interfere with each
other. For example, two of the apparently most important factors are
omega-3 fats (fish oil, etc.) and non-steroidal anti-inflammatory
medications (NSAIDs: aspirin, Motrin, etc.) are thought to have
beneficial effects due to their action on prostaglandins. However,
omega-3 fats are precursors to the prostaglandins, while NSAIDs stop
the conversion of precursors into prostaglandins. The effects of
combining the two are unclear. In this case, fortunately, there is a
prospective trial that partially answers the question, the Lyon Diet
Heart Study.11
To quote from this study in a discussion of the independent effects
of aspirin use, cholesterol, and hypertension, “the data indicate
that neither the Mediterranean dietary pattern nor any major bias has
altered the usual and expected relationships between the major risk
factors of CHD and recurrence.” (CHD = coronary heart disease).
Other evidence that combining the most important diet modifications
have added positive effects can be found in the following studies:
A
study of 7306 women followed for 31 years looked at “Risk
groups were defined using national guidelines for values of
systolic and diastolic blood pressure, serum cholesterol level,
body mass index, presence of diabetes, and smoking status.”
It showed that “for women with favorable levels for all
5 major risk factors at younger ages, CHD and CVD are rare;
long-term and all-cause mortality are much lower compared
with others.”12
One
study in short-lived, autoimmune disease-prone mice
showed that caloric restriction and fish oil had independent,
positive effects on life span. Either one by itself increased
life span of this mouse species by approximately 50%; combining
the two nearly doubled the life span (to near normal).13
n.b., this is NOT directly extensible to humans: both CR and fish
oil improve autoimmune conditions; this experiment has not been
repeated in normal mice.
Ross
and Bras showed that combining caloric restriction with
super-normal amounts of protein had an additive, positive effect
on life span.14
A
recent study from Oregon State University showed that
simultaneous supplementation with acetyl-L-carnitine
(ALCAR) and lipoic acid (LA) improves metabolic function while
reducing oxidative stress.15
In short, it improves mitochondrial function and decreases
mitochondrial damage from oxidation: these functions may
both improve function and extend life span (not proven yet to my
knowledge). Another study confirmed this simultaneous beneficial
effect on cognitive function in rats.16
Carnitine is found in meat and fish; LA is found in spinach. I do
not know if it best to supplement with ALCAR and LA (which I do
not), or to eat spinach and fish or meat frequently, but I like
the latter best. Juvenon is made up of these supplements. Another
study stated “After 25-month-old mice received basal diet
together with 300 mg/l acetyl L-carnitine in the drinking water
for 8 weeks, these levels were fully restored to those found in
younger animals. Dietary supplementation with melatonin or acetyl
L-carnitine partially reversed these changes. These findings
suggest that dietary supplementation cannot merely arrest but
indeed reverse some age-related increases in markers of oxidative
and inflammatory events occurring with the cortex.” 17
“Data
on the ingredients of the Polymeal were taken from the
literature. The evidence based recipe included wine, fish,
dark chocolate, fruits, vegetables, garlic, and almonds.
Data from the Framingham heart study and the
Framingham offspring study were used to build life
tables to model the benefits of the Polymeal in the
general population from age 50, assuming multiplicative
correlations. Results Combining the ingredients
of the Polymeal would reduce cardiovascular disease
events by 76%. For men, taking the Polymeal daily
represented an increase in total life expectancy of 6.6
years, an increase in life expectancy free from
cardiovascular disease of 9.0 years, and a decrease in
life expectancy with cardiovascular disease of 2.4
years. The corresponding differences for women were
4.8, 8.1, and 3.3 years.”18
Some
good web site sources for data used in this paper:
Harvard
School of Public Health: Nutrition Source.
http://www.hsph.harvard.edu/nutritionsource/
Frankly, this web site is as good as or better than whole
document that follows.
Keeping
Kids Healthy
(http://www.keepkidshealthy.com/welcome/bmicalculator.html)
– an outstanding, site including good objective information
and a calculator to figure out if your child is “at risk for
being overweight.”
PubMED
(http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=journals)
– Abstracts from all medical journals. Note: the quoted
articles have references primarily to these PubMED abstracts.
American
Journal of Clinical Nutrition (http://www.ajcn.org/)
Journal
of Nutrition (http://www.nutrition.org/)
Circulation
(http://circ.ahajournals.org/)
– Heart disease journal
Hypertension
(http://hyper.ahajournals.org/)
Stroke
(http://stroke.ahajournals.org/)
USDA
nutrient database
(http://www.nal.usda.gov/fnic/cgi-bin/nut_search.pl)
Eicosanoid
summary from the NIH (http://ods.od.nih.gov/eicosanoids)
American
Institute for Cancer Research (http://www.aicr.org/)
Merck
Manual (http://www.merck.com)
Botanical
list of food families
(http://www.calgaryallergy.ca/Articles/botanical.htm)
Go
to TOC
Meat
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Vegetarianism
|
Probably
has a small beneficial effect on lifespan
|
From
a well-thought out 2002 summary of many studies:
”-
vegetarians have low mortality compared with the general
population
- much of this benefit is attributable to
non-dietary lifestyle factors such as the avoidance of smoking and
a high socio-economic status
- vegetarians have similar
mortality to comparable non-vegetarians, although a vegetarian
diet may confer an additional 1-2 years of life (at least among US
Adventists).”
|
19
|
|
|
|
Less
risk of one type of kidney stones
|
About 12% of
kidney stones are from uric acid; gout is also caused by this.
Uric acid comes mostly from meat. “The results indicate that the
intake of a balanced vegetarian diet with a moderate animal
protein and purine content, an adequate fluid intake and a high
alkali-load with fruits and vegetables results in the lowest risk
of uric acid crystallization compared to the omnivorous diets.”
|
20
|
|
|
Meat
|
Increased
risk cardiovascular mortality from meat
|
A meta-analysis
of 5 large prospective “Western diet” vegetarian studies
showed that cardiovascular mortality is about 24% lower in
vegetarians. (from other studies, part of this may be due to lower
BMI)
|
21
|
|
|
|
Very
low meat intake is associated with longer life expectancy
|
Review
article: Very low meat intake is associated with longer life by
3.6 years. This effect may be at least partially due to factors
other than meat: those with low meat intake also tend to be
thinner and eat more healthy vegetables & nuts.
|
22
|
|
|
|
Increased
risk of gout, especially from red meat and beer; skim milk
decreases the risk.
|
“The
multivariate relative risk of gout among men in the highest
quintile of meat intake, as compared with those in the lowest
quintile, was 1.41… and the corresponding relative risk
associated with seafood intake was 1.51 … In contrast, the
incidence of gout decreased with increasing intake of [low fat]
dairy products; the multivariate relative risk among men in the
highest quintile, as compared with those in the lowest quintile,
was 0.56…The level of consumption of purine-rich vegetables and
the total protein intake were not associated with an increased
risk of gout.”
From
the 2004-03-13 Science News summary of the article, each daily
serving of meat increased gout risk by 21%, while each daily
fish serving increased the risk by 7%. In addition, each daily
serving of beer increased risk by 49%. Skim milk decreases the
risk by 21% per daily serving.
|
23
|
|
|
|
Increased
risk for diabetes (type 2, adult onset)
|
“We
prospectively assessed the associations between major dietary
patterns and risk of type 2 diabetes in women. Dietary information
was collected in 1984, 1986, 1990, and 1994 from 69 554 women aged
38 to 63 years without a history of diabetes, cardiovascular
disease, or cancer in 1984. We conducted factor analysis and
identified 2 major dietary patterns: "prudent" and
"Western." We then calculated pattern scores for each
participant and examined prospectively the associations between
dietary pattern scores and type 2 diabetes risks. RESULTS: The
prudent pattern was characterized by higher intakes of fruits,
vegetables, legumes, fish, poultry, and whole grains, while the
Western pattern included higher intakes of red and processed
meats, sweets and desserts, french fries, and refined grains.
During 14 years of follow-up, we identified 2699 incident cases of
type 2 diabetes. After adjusting for potential confounders, we
observed a relative risk for diabetes of 1.49 (95% confidence
interval [CI], 1.26-1.76, P for trend, <.001) when comparing
the highest to lowest quintiles of the Western pattern. Positive
associations were also observed between type 2 diabetes and red
meat and other processed meats. The relative risk for diabetes
for every 1-serving increase in intake is 1.26 (95% CI, 1.21-1.42)
for red meat, 1.38 (95% CI, 1.23-1.56) for total processed meats,
1.73 (95% CI, 1.39-2.16) for bacon, 1.49 (95% CI, 1.04-2.11) for
hot dogs, and 1.43 (95% CI, 1.22-1.69) for processed meats.”
|
24
|
|
|
|
Hypertension
|
“Compared
with quintile 1, the relative hazards of EBP for
quintiles 2–5 of plant food intake were 0.83 (95% CI:
0.68, 1.01), 0.83 (0.67, 1.02), 0.82 (0.65, 1.03), and 0.64
(0.53, 0.90), respectively; P for trend = 0.01…
positive dose-response relations for EBP were observed
across increasing quintiles of meat intake (P
for trend = 0.004).”
|
25
|
|
|
Red
meat
|
Colorectal
cancer
|
“N-Nitroso
compounds are suspected colorectal cancer (CRC) carcinogens to
which individuals on a diet high in red meat (RM) may be
particularly exposed… These data provide additional support for
the hypothesis that nitrosamines are carcinogenic to the rectum in
humans and that RM and, in particular, [processed meats] are
significant sources of exposure for these compounds.”
|
26
|
|
|
|
Increases
risk of colorectal cancer
|
An NIH study
found that the factors making the most difference are eating red
meat (OR [odds ratio] = 2.0), pan-fried red meat (OR = 2.0) and
well-done meat (OR = 1.7)
|
27
|
|
|
|
Increases
risk of colorectal cancer
|
A meta-analysis
of 13 studies found that “a daily increase of 100 g
of all meat or red meat is associated with a significant
12–17% increased risk of colorectal cancer” and that the
risk for processed meat was greater: “A significant
49% increased risk was found for a daily increase of 25
g of processed meat.”
|
28
|
|
|
|
Increased
risk of diabetes type 2
|
“Heme-iron
intake from red meat sources is positively associated with the
risk of type 2 diabetes. Total iron intake, heme-iron intake from
non-red meat sources, and blood donations are not related to the
risk of type 2 diabetes.” (relative risk = 1.63, i.e. a 63%
increased risk)
|
29
|
|
|
|
Increased
risk of rheumatoid arthritis
|
“A study of 25
000 people living in Europe shows that those who ate the most red
meat had double the risk of rheumatoid arthritis, compared to
those who ate the least amount. And people
who ate more protein overall, including other forms of meat and
plant protein, also had a higher risk of the disease while eating
fat did not seem to raise the risk, the researchers found.”
|
30
|
|
|
|
US
Government collusion in disinformation
|
“I first became
aware of the food industry as an influence on government nutrition
policies and on the opinions of nutrition experts when I moved to
Washington, DC, in 1986 to work for the Public Health Service. My
job was to manage the editorial production of the first-and as yet
only-Surgeon General's Report on Nutrition and Health, which
appeared as a 700-page book in the summer of 1988. This report was
an ambitious government effort to summarize the entire body of
research linking dietary factors such as fat, saturated fat,
cholesterol, salt, sugar, and alcohol to leading chronic diseases.
My first day on the job, I was given the rules: No matter what the
research indicated, the report could not recommend "eat less
meat" as a way to reduce intake of saturated fat, nor could
it suggest restrictions on intake of any other category of food.
In the industry-friendly climate of the Reagan administration, the
producers of foods that might be affected by such advice would
complain to their beneficiaries in Congress, and the report would
never be published.
This scenario was
no paranoid fantasy; federal health officials had endured a
decade of almost constant congressional interference with their
dietary recommendations. As I discuss in Part I, agency
officials had learned to avoid such interference by resorting to
euphemisms, focusing recommendations on nutrients rather than on
the foods that contain them, and giving a positive spin to any
restrictive advice about food. Whereas "eat less beef"
called the industry to arms, "eat less saturated fat"
did not. "Eat less sugar" sent sugar producers right to
Congress, but that industry could live with "choose a diet
moderate in sugar." When released in 1988, the Surgeon
General's Report recommended "choose lean meats" and
suggested limitations on sugar intake only for people particularly
vulnerable to dental cavities.”
|
31
|
|
|
Bacon
|
Increased
risk of bladder cancer
|
“In these 2
cohorts combined, frequent consumption of bacon was associated
with an elevated risk of bladder cancer.” (about double)
|
32
|
|
Go
to TOC
Inflammation
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Aspirin
|
Cardiovascular
disease
|
There
is no evidence that aspirin helps if you have low cardiovascular
risk factors.
|
33
|
|
|
|
Cardiovascular
disease
|
Aspirin
only helps those with high risk factors for MI. “For 1000
patients with a 5% risk for coronary heart disease events over 5
years, aspirin would prevent 6 to 20 myocardial infarctions but
would cause 0 to 2 hemorrhagic strokes and 2 to 4 major
gastrointestinal bleeding events. For patients with a risk of 1%
over 5 years, aspirin would prevent 1 to 4 myocardial infarctions
but would cause 0 to 2 hemorrhagic strokes and 2 to 4 major
gastrointestinal bleeding events.”
|
34
|
|
|
|
Cancer
(colon etc.)
|
Aspirin
may help prevent digestive tract cancer. “The role of aspirin on
the risk of cancers of the upper aerodigestive tract was
investigated in the combined data of three Italian case-control
studies, including 965 cases and 1779 hospital controls. The odds
ratio was 0.33 for users of >/=5 years, and 0.51 for >/=5
years since first use.”
|
35
|
|
|
|
Colon
cancer
|
A
randomized trial of patients who had previous colon adenomas
showed that “Low-dose aspirin has a moderate chemopreventive
effect on adenomas in the large bowel.” However, as noted in an
editorial in the same journal “The cumulative risk of major
adverse effects most likely outweighs any benefit in the
prevention of colorectal cancer, particularly when prevention due
to screening is considered.”
|
36
|
|
Go
to TOC
Glycation,
Advanced Glycation Endproducts (AGEs), and cooking methods
Direct,
non-enzymatic glycation damages your body tissue. This is what makes
diabetics age so quickly. A recent English study suggests that even
small elevations in blood sugar level (as measured via hemoglobin
A1C, or HbA1C for short) have a large effect on
the risk for heart attack. Glycation is simply the direct chemical
reaction between glucose in your blood stream (from carbohydrates
such as sugar, starches, fruits etc.) and your body's proteins. In
college chemistry, you may have heard of this as the Maillard
reaction. This reaction results in the proteins being degraded and
losing their function: tissues become stiff, arteries hard, lenses
opaque, spots form on your skin. This reaction is directly related to
the glucose concentration in the blood, which is a complex
interaction between what and when you eat, your body weight and body
fat, your activity level, your body's insulin response, etc. This is
too complex for me to sort out completely, but two things are clear
(for non-diabetics): insulin responsiveness declines in obese people,
and the glucose level rises fast after eating a lot of simple sugars
(a soda, fruit juice, ice cream, etc.) Therefore, simply keep slender
and avoid large quantities of sweets, just like your mother told you.
Another approach is to eat many small meals each day instead of one
or two large meals, to keep the peak glucose load down.
Glycation
also occurs in the intestines and outside the body, and that the
glycated proteins are readily absorbed. Thus, it is best to not
marinate meat with fruit or in sugary liquids. I like plain soy sauce
my self (or better, potassium chloride (KCl)). The most important and
straightforward way to reduce glycation is caloric restriction. If
you do nothing else, do this.
Advanced
Glycation End-products (AGEs) are the ultimate end waste product of
glycation damage. They form in the body, but also are present in
cooked fats and proteins. The most important and straightforward ways
to reduce AGE intake are 1) caloric restriction, 2) reduction of
cooking time and temperature, especially for fats and proteins, and
3) avoidance of cooked fatty foods. See the “AGE” tab of the
“Foods.xls” spreadsheet for the proportion of AGEs per 200
calories in some foods.
|
Glycation
related to aging
|
|
“Glycation, a
deleterious form of post-translational modification of
macromolecules has been linked to diseases such as diabetes,
cataract, Alzheimer's, dialysis related amyloidosis (DRA),
atherosclerosis and Parkinson's as well as physiological aging…
Macromolecular damage and biochemical changes that occur in aging
and age-related disorders point to the process of glycation as the
common event in all of them. This is supported by the fact that
several age-related diseases show symptoms manifested by
hyperglycemia.”
|
37
|
|
|
AGE
formation
|
CR
is the most effective way to reduce this
|
“…These
results suggest that long-term feeding of specific dietary
carbohydrates does not alter serum glucose concentrations or the
rate of collagen glycation. Rather, age-related accumulation of
AGE is more closely related to caloric intake.”
|
38
|
|
|
Advanced
glycosylation end-products (AGEs) in the diet
|
AGEs
can be absorbed when taken orally, and cause reduced insulin
sensitivity in mice
|
“AGEs are
abundant in exogenous sources such as foods, especially when
prepared under elevated temperatures (11,12). After ingestion, 10%
of preformed AGEs are absorbed into the human or rodent
circulation (13,14), of which two-thirds are retained in tissues…
reduced intake of dietary AGEs has been recently shown to decrease
the incidence of type 1 diabetes in NOD mice (26) as well as the
formation of atherosclerotic lesions in diabetic apolipoprotein
E-deficient mice”
|
39
|
|
|
|
Dietary
AGE has a large effect
|
Low
AGE in the diet was achieved by using different cooking methods:
“To vary the AGE content, foods, particularly meat, were exposed
to different cooking methods. L-AGE subjects were instructed to
boil, poach, stew or steam, avoid fried entrees, and reheat food
indirectly using steam in a double boiler.” This cut their
circulating AGE levels by 55%.
“…dietary glycotoxins contribute significantly to the
elevated AGE levels in renal failure patients. Moreover, dietary
restriction of AGE is an effective and feasible method to reduce
excess toxic AGE and possibly cardiovascular associated
mortality.”
|
40
|
|
|
|
|
“Foods
of the fat group showed the highest amount of AGE content with
a mean of 100+/-19 kU/g. High values were also observed for the
meat and meat-substitute group, 43+/-7 kU/g. The carbohydrate
group contained the lowest values of AGEs, 3.4+/-1.8 kU/g. The
amount of AGEs present in all food categories was related to
cooking temperature, length of cooking time, and presence of
moisture. Broiling (225 degrees C) and frying (177 degrees C)
resulted in the highest levels of AGEs, followed by roasting (177
degrees C) and boiling (100 degrees C).”
|
41
|
|
|
|
Dietary
AGE impairs wound healing
|
“Advanced
glycoxidation end products (AGEs) are implicated in delayed
diabetic wound healing. To test the role of diet-derived AGE on
the rate of wound healing, we placed female db/db (+/+) (n = 55,
12 weeks old) and age-matched control db/db (+/-) mice (n = 45) on
two diets that differed only in AGE content (high [H-AGE] versus
low [L-AGE] ratio, 5:1) for 3 months. Full-thickness skin wounds
(1 cm) were examined histologically and for wound closure...
L-AGE-fed mice displayed more rapid wound closure at days 7 and 14
(P < 0.005) and were closed completely by day 21 compared with
H-AGE nonhealed wounds. Serum AGE levels increased by 53% in H-AGE
mice and decreased by 7.8% in L-AGE mice (P < 0.04) from
baseline. L-AGE mice wounds exhibited lower skin AGE deposits,
increased epithelialization, angiogenesis, inflammation,
granulation tissue deposition, and enhanced collagen organization
up to day 21, compared with H-AGE mice. Reepithelialization was
the dominant mode of wound closure in H-AGE mice compared with
wound contraction that prevailed in L-AGE mice. Thus, increased
diet-derived AGE intake may be a significant retardant of wound
closure in diabetic mice; dietary AGE restriction may improve
impaired diabetic wound healing.”
|
42
|
|
|
AGE
absorption from foods
|
Cooking
at high temperatures or with simple sugars produces absorbable
AGEs
|
“To assess the
kinetics of ingested AGEs, investigators at this center recently
prepared, for five healthy persons and 38 diabetic patients with
or without overt renal disease, a breakfast consisting of 56 gm of
egg white cooked with or without 100 gm of fructose for one to
three hours at 90°C. In the cooked fructose-containing
mixture, the AGE content was more than 200 times that of the other
food. Over the ensuing 48 hours, blood and urine were sampled. The
high-AGE meal produced serum AGE elevations well correlated with
severity of renal disease. In particular, renal clearance ranged
from about 30% of absorbed AGEs in controls to less than 5% in
diabetic patients with renal failure. The rest was retained in the
body. Serum AGE analyses confirmed the ability of the absorbed
AGEs to crosslink biologic macromolecules (in this case,
radiolabeled fibronectin).
It must
immediately be said that the AGE content of one or another food
has no simple relation to its sugar content. The more important
relation is with the method of food preparation. Since the turn of
the 20th century, food chemists have appreciated that the changes
responsible for increasing the AGE content of a food--changes
known to them as the Maillard reaction and to the rest of us, less
formally, as the browning of raw foods by methods such as roasting
or braising--depend directly on temperature and are greatly
heightened by long exposure to high heat. Unfortunately, heat
creates tastes that humans enjoy, or at least tastes for which
humans in Western societies have developed an appetite. In recent
decades, food manufacturers have been using their knowledge of
Maillard chemistry to add appeal to natural foods and even to
incorporate such appeal into synthetic foods (an example being the
use of caramelized sugars in beverages such as Coca Cola). In
consequence, the AGE content of the Western diet has increased
vastly in the past 50 years.
A
few representative measurements may serve to illustrate the
importance of cooking method. So far, our group has analyzed 300
to 400 foods, using an immunoassay that assesses a few of the many
lipid- and protein-bound AGEs. By this test, roasted duck skin
(220°C for 110 minutes) exhibited, weight for weight, almost
15 times the AGE content of a doughnut (160°C for five
minutes). Cooking increased the doughnut's AGE content 24-fold and
the duck skin's 101-fold.”
|
43
|
|
|
|
Technical
discussion of AGE
|
Free pdf paper at
http://www.mssm.edu/msjournal/70/70_4_pages_232_241.pdf
A popular
discussion from the same author is at CBSnews: “The key to
lowering AGEs, said Vlassara, is to cook for a short time in the
presence of high humidity. This means either boiling or steaming
meats for the minimum time required. Meat can be sautéed,
she said, but it should be cut very thin and cooked quickly with a
small amount of oil.
She said one of the worst AGE offenders
is turkey cooked in the traditional American way.
"We
cook for many hours," she said. "That would tend to make
a tremendous number of AGEs.”
|
44
|
|
|
|
|
High AGE diet led
to kidney damage in diabetic and normal mice.
|
45
|
|
|
High
HbA1c is associated with vessel disease
|
Glycosylation
results in carotid plaques, even in normal, non-diabetic people
|
“HbA1c
measurements and ultrasonography of the carotid artery were
performed in 5960 subjects (3026 women, 2934 men) 25 to 84 years
of age...HbA1c was categorized into 5 groups: <5.0%, 5.0% to
5.4%, 5.5% to 5.9%, 6.0% to 6.4% and >6.4%. Carotid plaque
prevalence increased with increasing HbA1c level (P for linear
trend=0.002). The OR for hard plaques versus no plaques was 5.8
in the highest HbA1c group (>6.4%) compared with subjects in
the lowest group (<5.0%) after adjustment for several
possible confounders. The risk of predominantly hard plaques was
also significantly associated with HbA1c levels, although the ORs
at each level were somewhat lower than for hard plaques…
CONCLUSIONS: Metabolic changes reflected by HbA1c levels may
contribute to the development of hard carotid artery plaques, even
at modestly elevated levels.”
|
46
|
|
|
|
|
“Glycosylated
hemoglobin is an easily measured bio-chemical marker that strongly
correlates with the level of ambient glycemia during a 2- to
3-month period… Khaw and colleagues (14) carefully analyzed the
relationship of 1 hemoglobin A1c measurement to incident
cardiovascular events in a 6-year cohort study of 10 232 diabetic
and nondiabetic men and women age 45 to 79 years. After adjustment
for systolic blood pressure, cholesterol level, body mass index,
waist-to-hip ratio, smoking, and previous myocardial infarction or
stroke, there was a 21% increase in cardiovascular events for
every 1–percent-age point increase in hemoglobin A1c level above
5% (P 0.001). Similar relationships were observed for total
mortality (22% for men [P 0.001] and 28% for women [P
0.01] per 1–percentage point increase in hemoglobin A1c level).”
|
47
48
|
|
|
High-normal
glucose levels
|
Associated
with higher risk of death
|
“Using the
Framingham Heart Study data... After adjustment for systolic blood
pressure, cholesterol, body mass index, cigarette smoking, and use
of antihypertensive agents, they found that glucose was a strong,
independent predictor of mortality… For men, adjusted
mortality risk increased very rapidly through the normal range
(from 4.12% at 3.89 mmol/liter (70 mg/dl) to 12.26% at 5.55
mmol/liter (100 mg/dl)) and was flat at 12.26% thereafter. For
women, risk was flat at 3.65% through the normal range and then
increased rapidly, reaching 8.34% at 6.99 mmol/liter (126 mg/d),
but increased much more slowly thereafter. Exactly analogous
relations held for cardiovascular mortality. For men and women
combined, noncardiovascular mortality increased from 1.82% at 3.89
mmol/liter to 2.06% at 5.55 mmol/liter to 2.29% at 6.99 mmol/liter
(p for trend = 0.009). These findings suggest that although 5.55
mmol/liter (normal) may be a useful mortality risk division
(albeit with different implications for the two sexes), 6.99
mmol/liter (diabetic) is not, especially for men.”
|
49
|
|
|
Pyridoxamine
|
Inhibits
AGE formation
|
“[Pyridoxamine
(PM)] has a strong lipid-lowering effect in streptozotocin
(STZ)-induced diabetic and Zucker obese rats, and protects against
the development of nephropathy in both animal models. PM also
inhibits the development of retinopathy and neuropathy in the
STZ-diabetic rat.”
|
50
|
|
|
Benfotiamine
(a thiamine derivative)
|
AGE
prevention
|
Benfotiamine
blocks the formation of intracellular Advanced Glycation
Endproducts (AGE), through boosting the activity of the enzyme
transkelotase sufficiently to provide a metabolic "shunt"
for excess intracellular (as opposed to blood) glucose, reducing
the formation of highly reactive glycolytic intermediates called
triosephosphates. “…benfotiamine treatment … prevented
experimental diabetic retinopathy. The ability of benfotiamine to
inhibit three major pathways simultaneously might be clinically
useful in preventing the development and progression of diabetic
complications.”
|
51
|
|
|
Glucose
Alpha
lipoic acid
|
Increases
blood pressure & insulin resistance in rats
alpha
lipoic acid blocks this effect
|
Message:
avoid glucose (sugars & starches); consider using alpha lipoic
acid. “Chronic administration of glucose resulted in a 29%
increase in blood pressure, 30% increase in glycemia, 286%
increase in insulinemia, and 408% increase in insulin resistance
index. Chronic glucose feeding also resulted in a 22% greater
mitochondrial superoxide anion production in heart and in an
increase of 63% in AGE content in aorta. Increases in blood
pressure, aorta AGE content and heart mitochondrial superoxide
production were prevented in the rats fed glucose supplemented
with lipoic acid.”
|
52
|
|
|
Glycation
|
Strongly
correlated with carotid plaques
|
“HbA1c
was categorized into 5 groups: <5.0%, 5.0% to 5.4%, 5.5% to
5.9%, 6.0% to 6.4% and >6.4%. Carotid plaque prevalence
increased with increasing HbA1c level (P for linear trend=0.002).
The OR for hard plaques versus no plaques was 5.8 in the highest
HbA1c group (>6.4%) compared with subjects in the lowest group
(<5.0%) after adjustment for several possible confounders…
Metabolic changes reflected by HbA1c levels may
contribute to the development of hard carotid artery plaques,
even at modestly elevated levels.”
|
53
|
|
Go
to TOC
Carbohydrates
and insulin
One
term used in discussing glycation is “glycemic index”, or the
much more useful measurement of “glycemic
load”. Some foods with high
glycemic index and load include: all starches, potatoes, bread, rice,
sugar, honey, and breakfast cereals (except all-bran cereals); sweet
fruits also have a high glycemic load but have the benefit of
nutrients. This
web site has an extensive glycemic index list.
So note: In fact, the glucose load from starch-based foods like
bread, pizza, potatoes and noodles is equivalent to that from candy!!
Glycemic
load refers to how much your blood glucose level rises after eating
various foods. The glycemic load for sugar, rice, and bread would be
very high; for asparagus and peanuts very low. If you want to
minimize the glycation of your body’s tissues, practice caloric
restriction and eat foods with low glycemic loads (not too
much starch).
Fructose
(“fruit sugar”) is equally important to glucose in the problem of
glycation (J
Nutr 2000 May;130(5):1247-55; PMID: 10801926).
In lab rats it causes kidney damage and “…studies showed
that long-term fructose intake adversely affected several age-related
metabolic parameters.” (Kizhner
T, Werman MJ. Long-term fructose intake: Biochemical consequences and
altered renal histology in the male rat. Metabolism. 2002
Dec;51(12):1538-47. PMID: 12489065). Much
of it is (I think) converted to glucose quickly after ingestion. The
major sources of fructose in our diet are table sugar (half fructose
& half glucose), fruit, honey, and high-fructose corn syrup (corn
syrup is a part of many prepared foods at the grocery store such as
soft drinks, jams & yogurt). It is probably worth avoiding too
much of the sweet fruits, although berries (blueberries, raspberries,
strawberries, etc.) have much less sugar and seem to be fine.
Some
foods with low glycemic load include: onions, mushrooms, yams and
whole grain or 100% rye bread (pumpernickel are all good), but mostly
lots more vegetable 'fruits', i.e. peppers, tomato, cucumber, squash,
eggplant; cruciferous vegetables (cabbage, broccoli, cauliflower,
kale, Brussels sprouts); and leafy green vegetables of all kinds.
One
quick and easy way to effectively decrease the glycemic index of food
is to decrease the rate of gastric emptying. This can be done by
eating an acidic (e.g. a pickle, grapefruit juice, or a vinegar-based
dressing) or fatty food (e.g. nuts, fish) with your meals. High-fiber
food does not affect the glycemic index of a meal.
See
the Scientific American 2002-12 issue for an updated food pyramid
based on modern nutrition research.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Carbohydrates
|
Colon
cancer
|
There
may be an increased risk of colorectal cancer with high
carbohydrate intake. “increased eCarb and total carbohydrate
consumption are both associated with increased risk of CRC
[colorectal cancer] in both sexes, and that among women, relative
risk appears greatest for the right colon, whereas among men,
relative risk appears greatest for the rectum” (note: in
another careful case-control study, carbohydrates dropped out as a
risk factor in favor of calories)
|
54
|
|
|
|
Low-carbohydrate,
low iron, vegetable diet helps prevent progression of kidney
damage
|
“In
conclusion, [carbohydrate-restricted, low-iron-available,
polyphenol-enriched] CR-LIPE was 40-50% more effective than
standard protein restriction in improving renal and overall
survival rates.” (Polyphenols are found in tea, wine, etc.)
Although this is a study of kidney failure patients, the
implications may be much more widespread. Perhaps this type
of diet is healthy for other organs as well.
|
55
|
|
|
Blood
glucose level
|
Post-prandial
glucose level is more important than average
|
“Most
epidemiological data implicate postprandial hyperglycemia in the
development of cardiovascular disease, whereas the link between
fasting glycemia and diabetic complications is inconclusive.
Moreover, in many studies, postprandial glycemia is a better
predictor of cardiovascular risk than HbA(1c) level. Postprandial
glucose may have a direct toxic effect on the vascular
endothelium, mediated by oxidative stress that is independent of
other cardiovascular risk factors such as hyperlipidemia.”
|
56
|
|
|
|
High
levels damage mitochondria
|
“Four
main molecular mechanisms have been implicated in glucose-mediated
vascular damage. All seem to reflect a single
hyperglycaemia-induced process of overproduction of superoxide by
the mitochondrial electron-transport chain.”
|
57
|
|
|
|
Fasting
glucose >90, BMI >30, and triglyceride >150 =>
increased rate of subsequent diabetes
|
“We
obtained blood measurements, data from physical examinations, and
medical and lifestyle information from men in the Israel Defense
Forces who were 26 to 45 years of age. RESULTS: A total of 208
incident cases of type 2 diabetes occurred during 74,309
person-years of follow-up (from 1992 through 2004) among 13,163
subjects who had baseline fasting plasma glucose levels of less
than 100 mg per deciliter. A multivariate model, adjusted for age,
family history of diabetes, body-mass index, physical-activity
level, smoking status, and serum triglyceride levels, revealed a
progressively increased risk of type 2 diabetes in men with
fasting plasma glucose levels of 87 mg per deciliter (4.83 mmol
per liter) or more, as compared with those whose levels were in
the bottom quintile (less than 81 mg per deciliter [4.5 mmol per
liter], P for trend <0.001). In multivariate models, men with
serum triglyceride levels of 150 mg per deciliter …
combined with fasting plasma glucose levels of 91 to 99 mg per
deciliter …had a hazard ratio of 8.23 … for diabetes, as
compared with men with a combined triglyceride level of less than
150 mg per deciliter and fasting glucose levels of less than 86 mg
per deciliter … The joint effect of a body-mass index … of 30
or more and a fasting plasma glucose level of 91 to 99 mg per
deciliter resulted in a hazard ratio of 8….as compared with a
[BMI <] 25 and a fasting plasma glucose level of less than 86
mg per deciliter. CONCLUSIONS: Higher fasting plasma glucose
levels within the normoglycemic range constitute an independent
risk factor for type 2 diabetes among young men, and such levels
may help, along with body-mass index and triglyceride levels, to
identify apparently healthy men at increased risk for diabetes.”
|
58
|
|
|
Reduce
glycemic load (eat less non-fiber carbohydrates)
|
Reduces
heart attack risk
|
A
prospective study of 75,521 American women showed that those with
the lowest glycemic load had half the risk for heart attack of
women with the highest glycemic load.
|
59
|
|
|
|
Reduced
CRP level
|
Another
study showed that high glycemic load caused raised C-reactive
protein (CRP) levels. CRP is strongly correlated with heart attack
risk.
|
60
|
|
|
|
High
glycemic index and low cereal fiber diet are associated with Type
2 DM
|
From
the nurses health study: “After adjustment for age, body mass
index, family history of diabetes, and other potential
confounders, glycemic index was significantly associated with an
increased risk of diabetes (multivariate relative risks for
quintiles 1-5, respectively: 1, 1.15, 1.07, 1.27, and 1.59; 95%
CI: 1.21, 2.10; P for trend = 0.001). Conversely, cereal fiber
intake was associated with a decreased risk of diabetes
(multivariate relative risks for quintiles 1-5, respectively: 1,
0.85, 0.87, 0.82, and 0.64; 95% CI: 0.48, 0.86; P for trend =
0.004). Glycemic load was not significantly associated with risk …
CONCLUSIONS: A diet high in rapidly absorbed carbohydrates and
low in cereal fiber is associated with an increased risk of type 2
diabetes.”
|
61
|
|
|
|
High
GI and GL are associated with increased risk of prostate cancer
|
“ORs
[odds ratios] of prostate cancer and the corresponding 95% CIs
were derived using unconditional multiple logistic regression,
including terms for age, study center, education, family history
of prostate cancer, smoking, body mass index, physical activity,
alcohol consumption, intake of energy, fiber and lycopenes.
Compared to the lowest quintile of GI, the ORs were 1.23, 1.24,
1.47 and 1.57 for subsequent levels of GI. The corresponding
values for GL were 0.91, 1.00, 1.20 and 1.41…We found direct
relations between dietary GI and GL and prostate cancer risk.”
|
62
|
|
|
|
High
GL lowers HDL even in young people
|
“The
only significant correlations evident were negative correlations
between HDL cholesterol and glycemic load (in relation to white
bread), percentage carbohydrate, total dietary sugar, total
carbohydrate, and fructose. On stepwise multiple regression
analysis, glycemic load accounted for 21.1% of the variation in
HDL cholesterol.”
|
63
|
|
|
|
Reduces
stroke risk
|
“Cereal
fiber intake was inversely associated with total and hemorrhagic
stroke risk; for total stroke, relative risk = 0.66 (95%
confidence interval: 0.52, 0.83; p(trend) = 0.001) and for
hemorrhagic stroke, relative risk = 0.51 (95% confidence interval:
0.33, 0.78; p(trend) = 0.01). Findings suggest that high intake of
refined carbohydrate is associated with hemorrhagic stroke risk,
particularly among overweight or obese women. In addition, high
consumption of cereal fiber was associated with lower risk of
total and hemorrhagic stroke.”
Note:
The lifetime risk for stroke is about 20% for women and 10% for
men.
|
64
65
|
|
|
|
High
GI and GL (carbohydrate intake) ó
higher rate of cataracts
… Maybe.
I am not sure if they controlled for BMI etc.
|
“A
modified Block food-frequency questionnaire was used to obtain
dietary information from 3377 participants (aged 60-80 y; 56% were
women) in the Age-Related Eye Disease Study (AREDS)... RESULTS:
For participants in the highest quartile, dietary GI was
associated with a higher prevalence of all pure nuclear opacities
[grade >2; odds ratio (OR): 1.29; 95% CI: 1.04, 1.59; P for
trend = 0.02] and moderate nuclear opacities (grade >/=4; OR:
1.43; 95% CI: 0.96, 2.14; P for trend = 0.052). The OR in a
comparison of the highest with the lowest quartile of intake was
1.27 (95% CI: 0.99, 1.63; P for trend = 0.09) for cortical
opacities of any severity (>0% of area opaque), and the OR
increased somewhat for moderate cortical opacities (>5% of area
opaque; OR: 1.71; 95% CI: 1.00, 2.95; P for trend = 0.056).”
“Subjects
were 417 Boston-area members of the Nurses' Health Study cohort
aged 53-73 y... RESULTS: After multivariate adjustment, the odds
of cortical opacities (LOCS III >/=1.0) among women in the
highest tertile of carbohydrate intake (>/=200 g/d) was 2.46
times (95% CI: 1.30, 4.64; P for trend = 0.005) that among
women in the lowest tertile (<185 g/d).”
|
66
67
|
|
|
Glycemic
load
|
Increases
level of glucose in blood (bad)
|
“Stepwise
increases in glycemic load produced significant and predictable
increases in both glycemia (P < 0.001) and insulinemia (P <
0.001).”
An
interesting note: pasta has a relatively low glycemic index, while
potatoes and rice are very high.
|
68
|
|
|
Fructose
|
Causes
diabetes in rats
|
“Sprague-Dawley
rats fed a fructose-rich diet exhibit insulin resistance and
hypertension, a pathologic status resembling human type II
diabetes mellitus”
|
69
|
|
|
Insulin
score
|
Insulin
Index
|
Reducing
insulin response to foods may be as important as or more important
than reducing glycemic index.
|
70
|
Figure
|
|
Cut
down on sugars and fats
|
May
delay or reduce the disease of aging
|
“Simultaneous
consideration of the influence of the different types of
carbohydrates and fats in human diets on mortality rates
(especially the diseases of aging), and the probable retardation
of such diseases by caloric restriction (CR) leads to the
hypothesis that restriction of foods with a high glycemic index
and saturated or hydrogenated fats would avoid or delay many
diseases of aging and might result in life extension.”
|
71
|
|
|
|
May
reduce pancreas cancer risk
|
“The objective
of the study was to examine prospectively the association of the
consumption of added sugar (ie, sugar added to coffee, tea,
cereals, etc) and of high-sugar foods with the risk of pancreatic
cancer in a population-based cohort study of Swedish women and
men. DESIGN: A food-frequency questionnaire was completed in 1997
by 77 797 women and men aged 45-83 y who had no previous diagnosis
of cancer or history of diabetes. The participants were followed
through June 2005. RESULTS: During a mean follow-up of 7.2 y, we
identified 131 incident cases of pancreatic cancer. The
consumption of added sugar, soft drinks, and sweetened fruit soups
or stewed fruit was positively associated with the risk of
pancreatic cancer. The multivariate hazard ratios for the highest
compared with the lowest consumption categories were 1.69 (95% CI:
0.99, 2.89; P for trend = 0.06) for sugar, 1.93 (1.18, 3.14; P for
trend = 0.02) for soft drinks, and 1.51 (0.97, 2.36; P for trend =
0.05) for sweetened fruit soups or stewed fruit. CONCLUSION: High
consumption of sugar and high-sugar foods may be associated with a
greater risk of pancreatic cancer.”
|
72
|
|
Go
to TOC
Omega-3
fats
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Omega-3
fats
|
Cardiovascular
disease
|
“Randomized
trials have convincingly documented that omega-3 fatty acids can
significantly reduce the occurrence of CVD events in patients with
coronary artery disease. The strongest evidence to date is from
studies in which marine-derived omega-3 fatty acids have been
consumed as supplements or fish.”
|
73
|
|
|
|
|
The
AHA recommends that all adults eat fish (particularly fatty fish)
at least two times a week (fatty fish have the omega-3 fats DHA
and EPA). The AHA also recommends eating plant-derived omega-3
fatty acids (ALA, found in flax seed, canola oil, and walnuts).
|
74
|
|
|
|
Protect
against sudden death, NOT vs. atherosclerosis
|
“Both
clinical and animal-experimental evidence suggests that the effect
of n-3 PUFAs on the risk of sudden cardiac death relates primarily
to reduced vulnerability to ventricular fibrillation, rather than
to a reduction in atherosclerosis or nonfatal myocardial
infarction..”
|
75
|
|
|
|
Depression
|
“…percentages
of n-3 PUFAs and ratios of n-6 to n-3 PUFAs were significantly
lower and higher, respectively, in subjects with depressive
disorders than in control subjects…”
|
76
|
|
|
Fish
intake
|
Protects
against death in those with cardiovascular disease
|
“Compared
with no consumption, consumption of fish tended to be associated
with a lower risk of death [1–57 g/d, RR = 0.50 (0.20, 1.28); >
57 g/d, RR = 0.37 (0.14, 1.00); P for trend = 0.059].”
I.e.,
if you have CAD, eat ~3 oz of fish each day.
|
77
|
|
|
DHA
and EPA (long-chain omega 3 fats)
|
Help
infants develop neurologically
|
“A
prospective, double-blind, randomized controlled study was
conducted with 2 groups of healthy term infants [showed that]
Supplementation of healthy term infants with [long-chain
polyunsaturated fatty acids] during the first 2 mo of life reduces
the occurrence of mildly abnormal [general movements].”
|
78
|
|
|
|
Intake
of fish oil during pregnancy and lactation increases child’s IQ
|
A
randomized and double-blinded study of the effect of cod liver oil
supplementation (with DHA and EPA) “Children who were born to
mothers who had taken cod liver oil (n = 48) during pregnancy and
lactation scored higher on the Mental Processing Composite of the
K-ABC at 4 years of age as compared with children whose mothers
had taken corn oil (n = 36; 106.4 [7.4] vs 102.3 [11.3])… The
children's mental processing scores at 4 years of age correlated
significantly with maternal intake of DHA and eicosapentaenoic
acid during pregnancy… Maternal intake of very-long-chain n-3
PUFAs during pregnancy and lactation may be favorable for later
mental development of children.”
|
79
|
|
|
|
Help
prevent breast cancer
|
High
marine omega-3 (DHA and EPA) diet => 26% lesser risk of breast
cancer; high n-6 fat diet (e.g., corn oil) => 87% greater risk
of breast cancer.
|
80
|
|
|
DHA
|
Depression
|
The
omega-3 fat DHA found in fish may help prevent depression. “Mildly
depressed subjects had significantly reduced (-34.6%) adipose
tissue docosahexaenoic acid (DHA) levels than non-depressed
subjects. Multiple linear regression analysis indicated that
depression related negatively to adipose tissue DHA levels.”
|
81
|
|
Go
to TOC
Nuts
(see also Fats for the benefits of MUFA)
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Nuts
and monounsaturated fats
|
Cardiovascular
disease
|
“Nuts
such as pecans that are rich in monounsaturated fat may therefore
be recommended as part of prescribed cholesterol-lowering diet of
patients or habitual diet of healthy individuals.”
|
82
|
|
|
|
All-cause
mortality and ischemic heart disease (IHD)
|
“The
protective effect of nut consumption on IHD is not
offset by increased mortality from other causes.
Moreover, frequency of nut consumption has been found
to be inversely related to all-cause mortality in several
population groups such as whites, blacks, and the elderly.
Thus, nut consumption may not only offer protection
against IHD, but also increase longevity.” This
protection is 18% for those eating 1 oz of nuts every day, even
after all other factors are controlled for.
|
83
|
|
|
Nuts
|
Interesting
botany web site
|
Lots
of information and pictures at
http://waynesword.palomar.edu/ecoph8.htm
|
84
|
|
|
|
Reduce
incidence of gallstones
|
From
the Nurses’ Health Study: eating more than 5 oz of nuts/week
(either peanuts or other nuts) reduced the risk of cholecystectomy
by 25%.
|
85
|
|
|
|
|
In
a prospective long-term study, nuts and peanuts were both found to
be associated with reduced incidence of gallstones. “After
adjustment for age and other known or suspected risk factors, men
consuming 5 or more units of nuts per week… had a significantly
lower risk of gallstone disease (relative risk = 0.70…) than did
men who never ate or who ate less than 1 unit per month … (1
unit = 1 ounce (0.028 kg) of nuts).”
|
86
|
|
|
|
Reduce
bad lipids (LDL cholesterol)
|
A
systematic review of human studies showed: “The
results of 3 almond (50–100 g/d), 2 peanut (35–68 g/d),
1 pecan nut (72 g/d), and 4 walnut (40–84 g/d) studies
showed decreases in total cholesterol between 2 and 16% and
LDL cholesterol between 2 and 19% compared with subjects
consuming control diets. Consumption of macadamia nuts
(50–100 g/d) produced less convincing results. In
conclusion, consumption of
 50–100
g (1.5–3.5
servings) of nuts 50–100
g (1.5–3.5
servings) of nuts
 5
times/wk as part of a heart-healthy diet with total fat
content (high in mono- and/or polyunsaturated fatty
acids) of
35%
of energy may significantly decrease total cholesterol
and LDL cholesterol in normo- and hyperlipidemic
individuals.” 5
times/wk as part of a heart-healthy diet with total fat
content (high in mono- and/or polyunsaturated fatty
acids) of
35%
of energy may significantly decrease total cholesterol
and LDL cholesterol in normo- and hyperlipidemic
individuals.”
|
87
|
|
|
|
Eating
nuts does NOT tend to cause weight gain
|
“Review
of the available data to date suggests that adding nuts to
habitual diets of free-living individuals does not cause weight
gain. In fact, nuts have a tendency to lower body weight and fat
mass. In the context of calorie-restricted diets, adding nuts
produces a more lasting and greater magnitude of weight loss
among obese subjects while improving insulin sensitivity… there
is sufficient evidence to promote the inclusion of nuts as part of
healthy diets.”
|
88
|
|
|
Walnuts
|
Cardiovascular
disease
|
Walnuts
help prevent cardiovascular disease. “This study demonstrated
that walnuts, when consumed as part of a low fat, low-cholesterol
diet, have a beneficial effect on serum cardiovascular risk
factors.”
|
89
|
|
|
|
Protects
the heart
|
“Substituting
walnuts for monounsaturated fat in a Mediterranean diet improves
endothelium-dependent vasodilation in hypercholesterolemic
subjects. This finding might explain the cardioprotective effect
of nut intake beyond cholesterol lowering.”
|
90
|
|
|
Almonds
|
Almond
intake improves lipid profile
|
“Isoenergetic
incorporation of
 68
g of almonds (20% of energy) into an 8368-kJ (2000-kcal) Step I
diet markedly improved the serum lipid profile of healthy and
mildly hypercholesterolemic adults.” 68
g of almonds (20% of energy) into an 8368-kJ (2000-kcal) Step I
diet markedly improved the serum lipid profile of healthy and
mildly hypercholesterolemic adults.”
|
91
|
|
|
|
Help
with dieting
|
“[Low
calorie diet] supplementation with almonds, in contrast to complex
carbohydrates, was associated with greater reductions in
weight/BMI (-18 vs -11%), waist circumference (WC) (-14 vs -9%),
fat mass (FM) (-30 vs -20%) … and systolic blood pressure (-11
vs 0%)”
|
92
|
|
|
Macadamia
nuts
|
Favorably
affect blood lipid levels, and cholesterol in particular
|
My
take: nuts help against cholesterol, but you have to eat a lot.
“…macadamia nuts (40-90 g/d), equivalent to 15% energy intake…
Plasma total cholesterol and LDL cholesterol concentrations
decreased by 3.0 and 5.3%, respectively, and HDL cholesterol
levels increased by 7.9% in hypercholesterolemic men after
macadamia nut consumption.”
|
93
|
|
|
Peanuts
|
Cause
atherosclerosis in animals
|
“Peanut
oil is unexpectedly atherogenic for rats, rabbits, and primates.”
This is probably from the lectin content.
Additional
note: relative to other nuts, peanuts have less good MUFA and more
bad omega-6 fats.
|
94
95
|
|
Go
to TOC
Fats
(MUFA, saturated, and trans fats etc.)
Which
fats you eat and how much is very important. Also note that part of
the body’s response to diet modification is genetic (Am
J Clin Nutr 2002 Feb;75(2):191-212; PMID: 11815309).
In
summary:
BAD FATS: partially hydrogenated (“trans fats”),
saturated fats, and omega-6 (in large quantities)
GOOD FATS:
monounsaturated fats in moderate amounts, and omega-3 fats in small
quantities
HOW MUCH FAT TO EAT: 35% of calories (+/- 10%), as
part of a CR diet
BAD FATS
Definitely very
important: try to eliminate partially hydrogenated vegetable
oils. These have trans-fatty acids, shown to cause many health
problems: see Margarine,
Fatty Acids and Your Health.
Hydrogenation makes oils solid, but trans-fats are a NON-FOOD: they
are not easily metabolized in the body and accumulate over time,
increasing your risk for heart attack (Eur
J Clin Nutr 2000 Aug;54(8):618-25; PMID: 10951510).
They may also increase the risk of adult-onset diabetes (Dietary fat
intake and risk of type 2 diabetes in women. American Journal
of Clinical Nutrition, Vol. 73, No. 6, 1019-1026, June 2001.)
Eliminating these is very hard to do, as these make up margarine and
are the major fat used in most prepared foods such as cookies, cake
mixes, Raman noodles, bread, snacks, biscuits, etc. Read the
labels!
Cut down on animal fat (except fish), saturated
fats, and certain types of vegetable fats such as corn and safflower
oil (Am
J Clin Nutr 1999 Sep;70(3 Suppl):560S-569S; PMID: 10479232).
This will help reduce the incidence of stroke, heart attack, and
cancer.
The current Western diet is too rich in omega-6
fat from various vegetable sources,
and this is thought to cause much disease. Current theory is that
the ratio of omega-3 to omega-6 fat should be about 1 to 1; the
average Western diet has a ratio of about 1 to 15! (See either of
these National Institutes of Health sites discussing eicosanoids: 1
or 2)
In order to get some balance, eat some source of omega-3 fat. I know
of a few
sources: small, fatty, cold-water
fish (such as salmon,
herring, cod and sardines), perilla oil (whatever that is!) and flax
seed; there are probably several others. Corn,
sunflower, safflower, soy, sesame and cottonseed oils have lots of
omega-6 fat.
GOOD FATS
Modification of fat intake is far more important than how much
cholesterol you eat. What is good fat? Mono-unsaturated fats (MUFA)
and Omega-3 fats.
1. MUFA: Moderate quantities of
mono-unsaturated fats are good, especially those found in olive oil,
avocados, and nuts. [N.b., peanuts are not nuts but rather legume
seeds; while they have MUFAs they have been shown to cause
atherosclerosis (Lipids
1998 Aug;33(8):821-3; PMID: 9727614).]
A large study of 7th Day Adventists showed that the
lifetime risk of IHD was reduced by approximately 31% in those who
consumed nuts frequently (Am
J Clin Nutr 1999 Sep;70(3 Suppl):532S-538S; PMID: 10479227).
Another nut study showed a 47% reduction in sudden heart death in
those who ate nuts (Arch
Intern Med 2002 Jun 24;162(12):1382-7; PMID: 12076237).
A summary of data on nuts (Clin
Cardiol 1999 Jul;22(7 Suppl):III11-5; PMID: 10410300)
stated that "Four
of the best and largest cohort studies in nutritional epidemiology
have now reported that eating nuts frequently is associated with a
decreased risk of coronary heart disease of the order of 30-50%. The
findings are very consistent in subgroup analyses and unlikely to be
due to confounding. Possible mechanisms include reduction in LDL
cholesterol, the antioxidant actions of vitamin E, and the effects
on the endothelium and platelet function of higher levels of nitric
oxide." Another study showed that “Consumption
of nuts was also significantly associated with a reduced risk of
[Parkinson’s Disease] (for >/=5/week vs <1/month, pooled RR,
0.57; 95% CI, 0.34 to 0.95).” (Zhang
SM, Hernan MA, Chen H, Spiegelman D, Willett WC, Ascherio A. Intakes
of vitamins E and C, carotenoids, vitamin supplements, and PD risk.
Neurology. 2002 Oct 22;59(8):1161-9. PMID: 12391343.)
A study based on the Nurses’ Health Study
showed that eating an ounce of nuts 5 times each week reduces the
risk of type II diabetes by 27% (Jiang R, Manson JE, Stampfer
MJ, Liu S, Willett WC, Hu FB. Nut and Peanut Butter Consumption and
Risk of Type 2 Diabetes in Women.
JAMA. 2002;288:2554-2560) Another study showed
that substituting MUFA for saturated fats improved LDL levels and
insulin sensitivity (Vessby
B, Unsitupa M, Hermansen K, Riccardi G, Rivellese AA, Tapsell LC,
Nalsen C, Berglund L, Louheranta A, Rasmussen BM, Calvert GD,
Maffetone A, Pedersen E, Gustafsson IB, Storlien LH; KANWU Study.
Substituting dietary saturated for monounsaturated fat impairs
insulin sensitivity in healthy men and women: The KANWU Study.
Diabetologia. 2001 Mar;44(3):312-9. PMID: 11317662).
Caveat: a single study that was large,
multi-center, and case-controlled found an association between high
MUFA intake and macula degeneration (Arch
Ophthalmol 2001 Aug;119(8):1191-9; PMID: 11483088).
2.
Omega 3 fats (EPA and DHA) in moderation are particularly
important, as summarized in a review article (Am
J Clin Nutr 2000 Jan;71(1 Suppl):171S-5S; PMID: 10617967).
Fatty fish (e.g., salmon) has a large amount of omega 3 fat and is
probably good (Curr
Opin Lipidol 2001 Feb;12(1):11-7; PMID: 11176197).
EPA and DHA have beneficial anti-inflammatory effects; in people
“Clinical studies have reported that oral fish oil
supplementation has beneficial effects in rheumatoid arthritis and
among some patients with asthma, supporting the idea that the n-3
PUFA in fish oil are anti-inflammatory.” (Calder
PC. Dietary modification of inflammation with lipids. Proc Nutr Soc.
2002 Aug;61(3):345-58. Review. PMID: 12296294).
It even turns out that at least in mice fish fat does not induce
nearly as much weight gain or hyperglycemia as does lard, soybean
oil, or safflower oil (Metabolism
1996 Dec;45(12):1539-46; PMID: 8969289).
On the other hand, an older study from 1995 (N
Engl J Med 1995 Apr 13;332(15):977-82; PMID: 7885425)
found that protection from heart attacks by fish intake was the same
with 1 or 2 servings per week as with 5 or 6 servings per week (but
see below: too much may be bad!), and another found that fish eaten
1-3 times reduced the incidence of stroke by 43% (He
K, Rimm EB, Merchant A, Rosner BA, Stampfer MJ, Willett WC, Ascherio
A. Fish consumption and risk of stroke in men. JAMA. 2002 Dec
25;288(24):3130-6. PMID: 12495393).
Omega 3 fats probably protect against many, many diseases, including
dry eyes, breast
cancer, etc. EPA and DHA also
increase the flexibility of the arteries, reducing pulse pressure
and vascular resistance (Am
J Clin Nutr 2002 Aug;76(2):326-30; PMID: 12145002).
Studies show that omega-3 oil helps to prevent heart attacks and
probably
helps prevent depression or reduce bipolar psychosis.
A large, multi-center, case-controlled study (Arch
Ophthalmol 2001 Aug;119(8):1191-9; PMID: 11483088)
showed that fish oil reduces the rate of macula degeneration while
the omega-6 fat linoleic acid raises the risk, as does MUFA! The
American Heart Association (AHA) currently recommends two servings
per week of fatty fish (such as salmon). Note: because these oils
are polyunsaturated they are subject to very rapid oxidation both
outside and inside the body, and should always be used while still
quite fresh (mainly for flavor). They (i.e. canola oil and flax oil)
should not be used in cooking, as heat results in both still more
rapid oxidation and conversion to the trans- form.
A
meta-analysis of 11 randomized, controlled human trials with over
15,000 patients (Am
J Med 2002 Mar;112(4):298-304; PMID: 11893369)
found that “dietary and non-dietary intake of n-3 polyunsaturated
fatty acids reduces overall mortality, mortality due to myocardial
infarction, and sudden death in patients with coronary heart
disease.” (note, omega-3 is often abbreviated as n-3 or w-3.)
In addition, the type of omega-3 oil is important (EPA, DHA, and
alpha-linolenic acid (ALA) – see this description
of the essential fatty acids and deficiency symptoms).
EPA and DHA are long-chain omega-3 fats from fish, which in turn get
it from eating cold-water marine food. Most fresh fish in the store
is farm-raised fish, and some may have less EPA and DHA if they are
fed on corn or the like. A table of EPA and DHA content of
various fish can be found at:
http://groups.yahoo.com/group/crsociety/message/2946.
For psychological health it may be that the more EPA the
better, and the more DHA the worse. If you have problems with
depression, the best way of getting this ratio of omega-3 oil may be
to take a supplement such as OmegaBrite
(EPA to DHA ratio of 7:1), Omega-3s "700" (The Solgar
Vitamin Company), Pro-Omega from the company Nordic Naturals, GNC's
Fish Body Oils 1000 (30 percent concentrated omega-3 fatty acids,
with an EPA to DHA ratio of 1.5:1). For other health concerns,
salmon is just fine!
DHA
and EPA have also been associated with reduced ADHD
(hyperactivity / attention deficit disorder) in children – a real
breakthrough if this randomized prospective trial is confirmed!!
On the other hand, pregnant and nursing women probably need more
DHA and should consider increasing intake of certain fatty fish,
especially the wild salmon such as is found in canned salmon
products. These fish have high DHA levels, critical to the
development of the fetus and infant’s brain. A recent study showed
that breast-feeding is associated with enhanced stereopsis at age
3.5 y, as is a maternal DHA-rich antenatal diet, irrespective of
later infant feeding practice (Williams
C, Birch EE, Emmett PM, Northstone K; Avon Longitudinal Study of
Pregnancy and Childhood Study Team. Stereoacuity at age 3.5
y in children born full-term is associated with prenatal and
postnatal dietary factors: a report from a population-based cohort
study. Am J Clin Nutr. 2001 Feb;73(2):316-22. PMID:
11157330 full
text).
“Maternal intake
of very-long-chain n-3 PUFAs during pregnancy and lactation may be
favorable for later mental development of children.” Helland
IB, Smith L, Saarem K, Saugstad OD, Drevon CA. Intakes of
essential n-6 and n-3 polyunsaturated fatty acids among pregnant
Canadian women. Am J Clin Nutr. 2003 Feb;77(2):473-8. PMID:
12540410
“Pregnant and
nursing women should be encouraged to consume seafood on a regular
basis during pregnancy and lactation to furnish DHA for their
infants” Nettleton JA. Are n-3 fatty acids essential
nutrients for fetal and infant development? J Am Diet Assoc. 1993
Jan;93(1):58-64. Review. PMID:
8417094
On the DOWN SIDE:
polyunsaturated fats (PUFAs) - and especially DHA from fish - can
cause increased lipid peroxidation: they are chemically prone to
oxidation. A diet rich in PUFAs “induces only after two
days an increase in oxidized LDL/PUFAs for a
factor up to two in young people and for a factor of more than two
in old individuals” (Ann
N Y Acad Sci 2002 Apr;959:30-44; PMID: 11976183).
Indeed, oxidation of DHA in the mitochondrial membranes may
be a prime cause of aging itself, and the level of DHA is lower in
species with long life spans. I do not know however whether
mitochondrial DHA or oxidized lipid levels are related to lipid
intake. Perhaps of significance, one study found that CR reduced the
mitochondrial DHA level (Biochem
Biophys Res Commun 1987 Jun 30;145(3):1185-91; PMID: 3606601).
ALA is from flax seed (highest concentration) and certain other
plant sources such as canola. (Note: canola is derived from the rape
seed plant: canola was bred to have a lower – but not absent –
level of a cardiac toxin.) ALA has been shown to reduce cardiac
death (J
Nutr Health Aging 2001;5(3):179-83; PMID: 11458289).
Flax oil has the potential problem of associated increased rates of
prostate cancer in four epidemiological studies. However, flax seed
per se (as opposed to flax oil) has additional benefits of lignans
and fiber that may make using freshly ground flax seed
helpful overall in a healthy diet, particularly for women. In
addition the studies showing problems were not controlled for proper
use of the flax. Neither flax nor canola oil should be used for
frying (use olive oil (best), or butter), nor should flax oil or
anything other than freshly ground forms be used. Otherwise the
risks may be increased due to oxidation of the oil. In addition, a
study showed that the benefit of the Mediterranean Diet (rich in
olive oil and fish) is at least in part from monounsaturated fatty
acids (MUFA) or ALA. So getting the shorter chain omega-3 fats from
vegetable sources probably does help, and the longer chain omega-3
fats from fish help even more.
The NIH has a table
of omega-3 vs. omega-6 fatty acids,
listed as short or long, 6 or 3 (slightly modified below).
Omega6
Fatty Acids
------------------
Linoleic
Acid (LA) ................. C18:2;9,12
Gamma
Linolenic Acid (GLA) .......... C18:3;6,9,12
Dihomogamma
linolenic Acid (DGLA).... C20:3n6
Arachidonic
Acid (AA) ............... C20:4n6
Omega
3 Fatty Acids
-------------------
Alpha
Linolenic Acid (ALA), (LNA) ... C18:3;9,12,15
Eicosapentaenoic
Acid(EPA) .......... C20:5n3
Docosahexaenoic
Acid (DHA) .......... C22:6n3
HOW
MUCH FAT TO EAT
Epidemiological studies show that the
countries that have the highest fat diet, such as the USA, UK and
Canada, have the highest incidence of Alzheimer’s disease, while
the countries with the lowest intake of fat (i.e., Japan, Nigeria and
China) have the lowest incidence. This correlation of Alzheimer’s
disease with high fat intake was recently confirmed in a controlled
study of patients genetically predisposed to Alzheimer’s, where low
fat intake reduced the incidence by 50%! (Archives of Neurology,
2002-08). In addition there are numerous studies indicating lower
risks of coronary artery disease with lower intake of certain fats -
particularly animal fat, dairy fat, hydrogenated vegetable fats,
tropical oils and egg yolks (Am
J Clin Nutr 2002 Feb;75(2):191-212; PMID: 11815309);
other studies show other positive effects of low fat intake (Clin
Immunol Immunopathol 1990 Jan;54(1):103-16; PMID: 2293903).
Still other studies find a higher rate of cancers (including prostate
Cancer
Epidemiol Biomarkers Prev 2002 Aug;11(8):719-25; PMID: 12163324)
is associated with high-fat diets, even “good” MUFA fats. Of note
is that this relationship is correlated with average body weight or
calorie intake, and if that were taken into account, fat intake might
drop out as a risk factor.
On the other hand, the amount of
good fat in your diet should perhaps be about 20 to 40% of
your total calories. In favor of the upper limit is that fat is more
efficiently metabolized than carbohydrate, and metabolism of certain
fats may produce fewer free radicals than that of carbohydrates. It
is also much easier to maintain a moderate-fat diet: people on a
low-fat diet tend to quit. In addition, low-fat diets are strongly
correlated with an increased rate of ischemic strokes (Proc
Nutr Soc 2002 May;61(2):287-98; PMID: 12133212, ).
My
guess is that it is best to have a “normal” (about 35% of
calories) intake of fat, but keep the total down by caloric
restriction (again this comes up!)
A recent comprehensive review of diet and heart disease
stated that “Compelling evidence from metabolic studies,
prospective cohort studies, and clinical trials in the past several
decades indicates that at least 3 dietary strategies are effective in
preventing CHD: substitute nonhydrogenated unsaturated fats for
saturated and trans-fats; increase consumption of omega-3 fatty acids
from fish, fish oil supplements, or plant sources; and consume a diet
high in fruits, vegetables, nuts, and whole grains and low in refined
grain products. However, simply lowering the percentage of energy
from total fat in the diet is unlikely to improve lipid profile or
reduce CHD incidence. Many issues remain unsettled, including the
optimal amounts of monounsaturated and polyunsaturated fats, the
optimal balance between omega-3 and omega-6 polyunsaturated fats, the
amount and sources of protein, and the effects of individual
phytochemicals, antioxidant vitamins, and minerals.”
(Hu FB, Willett WC. Optimal Diets for Prevention of Coronary
Heart Disease. JAMA 2002;288:2569-2578).
Of
interest, the Mediterranean diet found that the following six foods
led to reduction in risk of heart attacks, with the odds ratio given
last (Eur
J Nutr 41 (2002) 4, 153-160; PMID: 12242583).
They also noted that “our results support the
exclusion of refined cereals with a high glycaemic load as healthy
elements of this pattern.”
Food gm/day Odds
ratio
Olive
oil 10-18 0.34
Fiber 18-26
0.25
Fruit 365-570 0.32
Vegetables 482-583 0.36
Fish 77-106 0.28
Alcohol 0-7 0.49
Contraindications
to fat modification: None that I know of.
Potential problems: Too
much fish (of many types) is not good for children or potentially
pregnant women because of tiny amounts of mercury in fish. See this
FDA document (http://www.cfsan.fda.gov/~frf/sea-mehg.html)
for a list of mercury levels, or possibly this
EPA fish consumption advisory summary.
Avoid bottom-dwelling fish, fresh-water fish, bluefin tuna (albacore
too), mackerel, shark and tilefish (a.k.a. golden snapper): these
large fish that live long enough to accumulate quantities of mercury
and are thus potentially dangerous if you eat them frequently. Also
avoid tuna steaks (canned tuna is better but not perfect). The
Environmental Working Group says there are some fish considered safe
for pregnant women, including farm-raised trout and catfish, shrimp,
fish sticks, flounder (summer), wild pacific salmon, croaker,
mid-Atlantic blue crab and haddock. Indeed, salmon and shrimp have
almost no detectable mercury and are probably quite safe.
Reduce
intake of highly processed and junk foods, such as boxed cookies,
pudding mixes and fast food from places like McDonalds and Burger
King, etc. These tend to have high quantities of partially
hydrogenated oils, charred meat, and aluminum (an anti-caking agent
that may be associated with neurological problems; however, aluminum
is also found everywhere else including soil, cooking pots,
antiperspirants, and municipal drinking water)
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Fats
|
|
This
web site is an OUTSTANDING scientific summary of the various types
of fats, their sources, what fats are found in various foods, why
trans fats (partially hydrogenated oils) are bad, etc.
http://www.scientificpsychic.com/fitness/fattyacids.html
|
96
|
|
|
|
Use
MUFA fats and avoid saturated and trans-fats
|
A
meta-analysis of 60 controlled trials showed that the ratio of HDL
to total cholesterol was influenced by the type of fat eaten.
“Lauric acid [coconut oil] greatly increased total cholesterol,
but much of its effect was on HDL cholesterol. Consequently, oils
rich in lauric acid decreased the ratio of total to HDL
cholesterol. “ “… risk is reduced most effectively when
trans fatty acids and saturated fatty acids are replaced with cis
unsaturated fatty acids.”
|
97
|
|
|
|
Parkinson
disease
|
“Estimating
the association between PD [Parkinson disease] and risk of being
in the highest versus the lowest intake quartile, there were
elevated odds ratios for total fat (OR 1.94, 95% confidence
interval [CI] : 1.05-3.58), cholesterol (OR 2.11, 95% CI:
1.14-3.90), lutein (OR 2.52, 95% CI: 1.32-4.84) and iron
(OR 1.88, 95% CI: 1.05-3.38).” This study is from Detroit: most
of the fat and cholesterol is from animal fat. The lutein (from
broccoli and kale) correlation is somewhat worrisome.
|
98
|
|
|
Saturated
fat
|
Associated
with reduced bone density
|
“These
data indicate that [bone mineral density] is negatively associated
with saturated fat intake, and that men may be particularly
vulnerable to these effects.”
|
99
|
|
|
|
Increases
LDL cholesterol, worsens insulin resistance, increases cancer, may
cause brain function problems
|
This
site is a MSNBC nutrition article; basically a readable summary
that emphasizes that saturated fat is bad for health.
|
100
|
|
|
|
Raises
cholesterol
|
“Regression
analysis of the combined published data on the effects of
dietary fatty acids and cholesterol on serum cholesterol and
lipoprotein cholesterol evaluated with groups of human subjects
shows that 1) saturated fatty acids increase and are the primary
determinants of serum cholesterol, 2) polyunsaturated fatty acids
actively lower serum cholesterol, 3) monounsaturated fatty acids
have no independent effect on serum cholesterol and, 4) dietary
cholesterol increases serum cholesterol”
|
101
|
|
|
Saturated
and trans-fats
|
Alzheimer
disease increased
|
Trans
fats increase risk: “Risk … increased with consumption of
trans-unsaturated fats” (relative risk = 2.4)
Saturated
fats increase risk (relative risk = 2.2)
|
102
|
|
|
|
Increase
coronary heart disease
|
From
the Nurses' Health Study. “We prospectively studied 80,082 women
who were 34 to 59 years of age and had no known coronary disease,
stroke, cancer, hypercholesterolemia, or diabetes in 1980.
Information on diet was obtained at base line and updated during
follow-up by means of validated questionnaires. During 14 years of
follow-up, we documented 939 cases of nonfatal myocardial
infarction or death from coronary heart disease. Mutivariate
analyses included age, smoking status, total energy intake,
dietary cholesterol intake, percentages of energy obtained from
protein and specific types of fat, and other risk factors.
RESULTS: Each increase of 5 percent of energy intake from
saturated fat, as compared with equivalent energy intake
from carbohydrates, was associated with a 17 percent increase in
the risk of coronary disease (relative risk, 1.17; 95
percent confidence interval, 0.97 to 1.41; P=0.10). As compared
with equivalent energy from carbohydrates, the
relative risk for a 2 percent increment in energy intake from
trans unsaturated fat was 1.93 (95 percent confidence
interval, 1.43 to 2.61; P<0.001); that for a 5 percent
increment in energy from monounsaturated fat was 0.81 (95 percent
confidence interval, 0.65 to 1.00; P=0.05); and that for a 5
percent increment in energy from polyunsaturated fat was 0.62 (95
percent confidence interval, 0.46 to 0.85; P= 0.003). Total fat
intake was not signficantly related to the risk of coronary
disease (for a 5 percent increase in energy from fat, the relative
risk was 1.02; 95 percent confidence interval, 0.97 to 1.07;
P=0.55). We estimated that the replacement of 5 percent of
energy from saturated fat with energy from unsaturated fats would
reduce risk by 42 percent (95 percent confidence interval, 23
to 56; P<0.001) and that the replacement of 2 percent of energy
from trans fat with energy from unhydrogenated, unsaturated fats
would reduce risk by 53 percent (95 percent confidence interval,
34 to 67; P<.001). CONCLUSIONS: Our findings suggest that
replacing saturated and trans unsaturated fats with unhydrogenated
monounsaturated and polyunsaturated fats is more effective in
preventing coronary heart disease in women than reducing overall
fat intake.”
|
103
|
|
|
Animal
fat
|
Parkinson
disease greatly increased
|
“…increasing
intake of animal fats were strongly related to PD [Parkinson
disease] (odds ratio, 5.3; 95% confidence interval,
1.8-15.5; p for trend = 0.001).”
|
104
|
|
|
|
Saturated
fats reduce insulin sensitivity
|
SFA
(saturated fats) may thus be a cause of diabetes. “The plasma
insulin response was significantly higher following the SFA meal
than the other meals after both breakfast and lunch (P<0.006)
although there was no effect of breakfast fatty acid composition
on plasma glucose concentrations. Postprandial insulin sensitivity
(SI(Oral)) was assessed for 180 min after each meal. SI(Oral) was
significantly lower after lunch than after breakfast for all four
test meals (P=0.019) following the same rank order (SFA < n-6
PUFA < n-3 PUFA < MUFA) for each meal. The present study
demonstrates that a single meal rich in SFA
reduces postprandial insulin sensitivity with 'carry-over'
effects for the next meal.”
|
105
|
|
|
Trans
fat
|
Are
2.5 to 10 times worse for you than saturated fat!
|
“Compared
to saturated fat, TFAs [trans fatty acids] are, gram to gram,
associated with a considerably (2.5- to >10-fold) higher risk
increment for IHD.” (IHD = Ischemic Heart Disease). “Danish
government has decided that oils and fats containing more than 2%
industrially produced TFAs will not be sold in Denmark after the
January 1, 2004.”
|
106
|
|
|
|
Trans
fat sources
|
Margarine,
frosting, crackers, biscuits, cookies, cakes and other baked goods
all are bad sources. Approximately 21-36% of their fat is trans
fat (from USDA analysis). Of course, margarine is the most
concentrated form. If you use olive oil to bake something at home,
this is not a problem.
Note:
about 5% of fat from cows (in beef, milk, and butter) are trans
fats! This is based on USDA data. Thus, cow fat has about 1/5 of
the trans fat that margarine does. Even so, this trans fat
accounts for a large fraction of the heart risks from butterfat.
|
|
|
|
|
Increases
asthma
|
A
German survey found that “Frequent intake of margarine of any
kind was positively associated with current asthma during the past
12 months in young adults aged 18 to 29 years (aOR, 2.33; 95% CI,
1.03-5.26). In subgroup analysis, the positive association was
confined to frequent intake of low-fat margarine (4.51;
1.78-11.43) or the combination of low-fat margarine and low-fat
butter (4.79; 1.84-12.44). Consumption of margarine of any kind
was not related to hay fever, atopic dermatitis, and atopic
sensitization to inhalant allergens.” I do not know what
“low-fat margarine” is in the German context.
|
107
|
|
|
|
Bad
fats: Trans and saturated
Fat
should be 30-35% of energy intake
|
“there
is a general consensus concerning the need to decrease the intake
of trans and saturated fatty acids with regard to the risk of CHD”
“A modest reduction in fat intake to 30-35% energy, with the
bulk of carbohydrates being derived from complex carbohydrates
from unrefined sources, would appear to be the best option for the
prevention of obesity and cardiovascular disease.”
|
108
|
|
|
|
Good
fats: n-3, monounsaturated, CLA
n-6
is bad fats
|
Review:
“The cardioprotective effects of the long
chain n-3 PUFAs found in oily fish and fish oil [3] have been
confirmed by recent studies.” “A recent study reported
that the n-6 PUFA arachidonic acid can
induce the production of damaging proinflammatory cytokines”
|
109
|
|
|
Monounsaturated
fats (MUFA)
|
High-MUFA
diet helps lipid profiles in diabetics
|
“…17%
to 20% [of calories from] monounsaturated fat… [resulted in]
lower plasma total triglycerides by 18% (P=.027), lower very
low-density lipoprotein triglycerides by 26% (P=.043), lower very
low-density lipoprotein cholesterol by 48% (P=.043), higher
apolipoprotein A1 by 7% (P=.018), smaller low-density lipoprotein
particle size by 1% (P=.043), and longer low-density lipoprotein
oxidation lag time by 25% (P=.043) were found after the
high-monounsaturated-fat diet.”
|
110
|
|
|
|
Reduces
LDL cholesterol
|
“Plasma
cholesterol concentrations decreased in a dose-dependent
manner with increasing intakes of dietary MUFAs. This change
was entirely accounted for by reduced LDL cholesterol”
|
111
|
|
|
|
Reduces
clotting from two pathways
|
“In
conclusion, a high-MUFA diet sustains potentially beneficial
effects on platelet aggregation and postprandial activation of
factor VII.”
|
112
|
|
|
|
Reduces
lipid oxidation
|
Rats
given olive oil (MUFA) had less lipid oxidation than those given
sunflower seed oil (n-6 polyunsaturated). “In conclusion, the
type of dietary fat should be considered in studies on aging,
since oxidative stress is directly modulated by this factor.”
|
113
|
|
|
|
Reduced
triglyceride (TG)
|
Calories
from MUFA are better for you than calories from carbohydrate: “The
MUFA-rich diet showed better effects on serum TG than the
[carbohydrate]-rich diet, even with energy restriction and weight
loss.”
|
114
|
|
|
|
Reduced
arteriosclerosis risk
|
A
review states that “many observational epidemiological studies
suggest that a high intake of monounsaturated fat is associated
with reduced coronary risk”
|
115
|
|
|
|
Olive
oil
|
“Olive
oil supplementation alone improved the lipid profile but was more
effective when coupled with dietary restriction. There was a
synergistic beneficial action of dietary restriction and olive oil
on serum lipids and myocardial antioxidant defences.”
|
116
|
|
|
|
Reduced
mortality rate
|
“After
a median follow-up of 8.5 years, we investigated the possible role
of MUFA, PUFA, and other selected food groups in protecting
against all-causes mortality in a population-based, prospective
study, conducted in one of the eight centers of the Italian
Longitudinal Study on Aging (ILSA), Casamassima, Bari, Italy. Out
of 704 elderly subjects (65-84 years), 278 nondemented persons
agreed to participate at the first survey (1992-1993). During the
follow-up, there were 91 deaths. A semi-quantitative food
frequency questionnaire evaluating macronutrient daily intakes
were performed at the first survey. Higher MUFA intake was
associated with an increase of survival (hazard ratio 0.81, 95% CI
0.66-0.99),”
|
117
|
|
|
|
Reduced
Parkinson Disease
|
“In
the Rotterdam Study, a prospective population-based cohort study
of people ages > or =55, the association between intake of
unsaturated fatty acids and the risk of incident PD was evaluated
among 5,289 subjects who were free of dementia and parkinsonism
and underwent complete dietary assessment at baseline...After a
mean follow-up of 6.0 years, 51 participants with incident PD were
identified. Intakes of total fat, monounsaturated fatty acids
(MUFAs), and polyunsaturated fatty acids (PUFAs) were
significantly associated with a lower risk of PD, with an adjusted
hazard ratio per SD increase of energy-adjusted intake of 0.69
(95% CI 0.52 to 0.91) for total fat, of 0.68 (95% CI 0.50 to 0.94)
for MUFAs, and 0.66 (95% CI 0.46 to 0.96) for PUFAs. No
associations were found for dietary saturated fat, cholesterol, or
trans-fat. CONCLUSION: These findings suggest that high intake of
unsaturated fatty acids might protect against Parkinson disease.”
|
118
|
|
|
|
Reduced
blood pressure
|
“Randomized,
3-period, crossover feeding study … Participants were 164 adults
with prehypertension or stage 1 hypertension. Each feeding period
lasted 6 weeks and body weight was kept constant. INTERVENTIONS: A
diet rich in carbohydrates; a diet rich in protein, about half
from plant sources; and a diet rich in unsaturated fat,
predominantly monounsaturated fat. MAIN OUTCOME MEASURES: Systolic
blood pressure and low-density lipoprotein cholesterol. RESULTS:
Blood pressure, low-density lipoprotein cholesterol, and estimated
coronary heart disease risk were lower on each diet compared with
baseline. Compared with the carbohydrate diet, the protein diet
further decreased mean systolic blood pressure by 1.4 mm Hg (P
= .002) and by 3.5 mm Hg (P = .006) among those with hypertension
and decreased low-density lipoprotein cholesterol by 3.3 mg/dL
(0.09 mmol/L; P = .01), high-density lipoprotein cholesterol by
1.3 mg/dL (0.03 mmol/L; P = .02), and triglycerides by 15.7 mg/dL
(0.18 mmol/L; P<.001). Compared with the carbohydrate diet, the
unsaturated fat diet decreased systolic blood pressure by 1.3
mm Hg (P = .005) and by 2.9 mm Hg among those with
hypertension (P = .02), had no significant effect on low-density
lipoprotein cholesterol, increased high-density lipoprotein
cholesterol by 1.1 mg/dL (0.03 mmol/L; P = .03), and lowered
triglycerides by 9.6 mg/dL (0.11 mmol/L; P = .02). Compared
with the carbohydrate diet, estimated 10-year coronary heart
disease risk was lower and similar on the protein and unsaturated
fat diets.”
|
291259
|
|
|
 -linolenic
acid (GLA) from borage oil -linolenic
acid (GLA) from borage oil
|
Reduces
atopic dermatitis
|
“In
a double-blind, randomized, placebo-controlled trial… Early
supplementation with GLA in children at high familial risk does
not prevent the expression of atopy as reflected by total serum
IgE, but it tends to alleviate the severity of atopic dermatitis
in later infancy in these children.”
Note:
GLA is also found in pecans and walnuts.
|
119
|
|
|
Lecithin
|
Mitochondria
damage (aging)
|
Lecithin
(in the form of phosphatidyl choline) may reduce mitochondrial DNA
damage: if so, this one fact alone may be of great importance in
reducing the rate of aging. HOWEVER, this is not easily obtained
in the form and dosage used in the rodent experiments.
|
120
|
|
|
|
Low
insulin => low mitochondria ROS
|
In
a rat experiment, CR => lower mitochondrial reactive oxygen
species (mtROS); insulin reversed this. It MAY be that by keeping
insulin low (CR, low glycemic index, small meals etc.) we can
mimic or enhance the effects of CR
|
121
|
|
|
Omega
3
|
|
Omega
3 fats are associated with lower mortality in a very large
meta-analysis “a systematic search of randomized controlled
trials”; omega 3 fats out-performed statins! “Compared with
control groups, risk ratios for overall mortality were 0.87 for
statins (95% confidence interval [CI], 0.81-0.94), 1.00 for
fibrates (95% CI, 0.91-1.11), 0.84 for resins (95% CI, 0.66-1.08),
0.96 for niacin (95% CI, 0.86-1.08), 0.77 for n-3 fatty acids (95%
CI, 0.63-0.94), and 0.97 for diet (95% CI, 0.91-1.04)…CONCLUSIONS:
Statins and n-3 fatty acids are the most favorable lipid-lowering
interventions with reduced risks of overall and cardiac
mortality.”
|
122
|
|
|
Omega
3: ALA (short-chain) (?)
|
|
“Dietary
polyunsaturated and more specifically linoleic fatty acid intake
may have a substantial cardioprotective benefit that is also
reflected in overall mortality. Dietary fat quality seems more
important than fat quantity in the reduction of cardiovascular
mortality in men.”
|
123
|
|
|
Omega
3: DHA and EPA (long-chain)
|
DHA
/ fish oil may be harmful to lifespan, in theory
|
This
CR society e-mail summary by Michael Rae (AOR, Canada) explains
how DHA / fish oil may theoretically be harmful for life span of
very long life expectancy people, even if it is helpful for
cardiac disease in obese people. “Michael Rae's Fish oil
Accelerated Aging" (MiRFAA) hypothesis is based on the
mitochondrial free-radical theory of aging (MiFRA). I think this
might apply most to those who have a very long life expectancy
because of CR since youth combined with good nutrition and habits.
To
quote Michael Rae from a CR Society post of 2004-05-11:
“1.
Across species, double bond content in the mitochondrial (mt)
inner membrane (MIM) - and especially DHA content - is inversely
correlated with max LS.
2.
Within a species, double bond content in MIM increases with aging.
3.
CR, the only anti-aging therapy per se (only therapy which extends
max LS, maintains molecular fidelity, extends physiological
functioning, etc) in mammals, retards this increase, apparently by
lowering delta-5 desaturase activity & perhaps by modulatings
phospholipids acyltransferase activity.
4.
Feeding all animals yet tested longer-chain PUFA, such as DHA,
increases DHA content in MIM.
5.
This increase in MIM DHA increases the actual peroxidation of the
MIM.
Inductive
conclusion, from the above & a few other tidbits: eating DHA
will lead to more DHA in MIM; more DHA in MIM is in direct
opposition to a known effect of CR, and correlates with aging
within and across species.”
His
advice to those who practice CR: “So: don't eat DHA. Avoid fatty
fish, and don't take fish oil supplements.”
|
124
|
|
|
|
Fish
oil supplements do NOT have PCBs or mercury, two toxins present in
fish meat
|
“In
a previous study we showed that the amount of mercury in 5
over-the-counter brands of fish oil was negligible. …The levels
of polychlorinated biphenyls and organochlorines were all below
the detectable limit. CONCLUSIONS: Fish oil supplements are more
healthful than the consumption of fish high in organochlorines.
Fish oils provide the benefits of omega-3 fatty acids without the
risk of toxicity. In addition, fish oil supplements have been
helpful in a variety of diseases, including bipolar disorder and
depression.”
|
125
|
|
|
|
Fish
consumption is associated with less hostility in young adulthood!
|
From
an Oakland, California study: “…a sample of 3581 urban white
and black young adults… Consumption of any fish rich in n-3
fatty acids, compared to no consumption, was also independently
associated with lower odds of high hostility (OR=0.82; 95%
CI=0.69-0.97; P=0.02). These results suggest that high dietary
intake of DHA and consumption of fish rich in n-3 fatty acids may
be related to lower likelihood of high hostility in young
adulthood.”
|
126
|
|
|
|
EPA
may help treat depression and schizophrenia
|
“…we
investigated whether membrane concentrations of these fatty acids
might vary as a function of schizotypal traits in non-psychotic
individuals… Our findings … are quite consistent with evidence
that omega-3 fatty acids (notably EPA) can be useful in the
treatment of schizophrenic illness.”
“Four
out of five placebo-controlled double- blind trials of
eicosapentaenoic acid (EPA) in the treatment of schizophrenia have
given positive findings. In depression, two placebo-controlled
trials have shown a strong therapeutic effect of ethyl-EPA added
to existing medication.”
|
127
|
|
|
|
Improves
cardiovascular risk factors and disease
|
The
AHRQ (Agency for Healthcare Research and Quality,
http://www.ahrq.gov/clinic/epcindex.htm#dietsup)
review of very many of the largest randomized clinical trials
found that:
1.
Triglycerides: there is strong evidence
that fish oils have a strong beneficial
effect on (10-30%) that is dose-dependent
2.
Blood pressure: a very small beneficial effect (2 mm Hg)
3.
Cardiovascular mortality: there is evidence to support the
hypothesis that fish, fish oil, or ALA supplement consumption
reduces all-cause mortality and various CVD outcomes, although the
evidence is strongest for fish or fish oil.
It
does NOT help with cholesterol, HDL
cholesterol, LDL cholesterol, fasting blood sugar, or
glycosylated hemoglobin or insulin.
|
|
|
|
|
|
“A
meta-analysis of cohort studies was conducted to examine the
association between fish intake and CHD mortality…A database was
developed on the basis of 11 eligible studies and 13 cohorts,
including 222 364 individuals with an average 11.8 years of
follow-up… Each 20-g/d increase in fish intake was related to
a 7% lower risk of CHD mortality (P for trend=0.03).”
|
128
|
|
|
|
Fish
decreases the risk of stroke
|
A
meta-analysis of 9 cohort studies found that “intake of fish is
inversely related to risk of stroke, particularly ischemic
stroke.” “Compared with those who never consumed fish or ate
fish less than once per month, the pooled [relative risks] for
total stroke were 0.91 … for individuals with fish intake 1 to 3
times per month, 0.87 … for once per week, 0.82 … for 2 to 4
times per week, and 0.69 … for > or =5 times per week (P for
trend=0.06).”
|
129
|
|
|
|
|
Do
not eat fried fish or fish sandwiches. “In multivariate
analyses, tuna/other fish consumption was inversely associated
with total stroke (P = .04) and ischemic stroke (P = .02), with
27% lower risk of ischemic stroke with an intake of 1 to 4 times
per week (hazard ratio [HR], 0.73; 95% confidence interval [CI],
0.55-0.98) and 30% lower risk with intake of 5 or more times per
week (HR, 0.70; 95% CI, 0.50-0.99) compared with an intake of less
than once per month. In contrast, fried fish/fish sandwich
consumption was positively associated with total stroke (P = .006)
and ischemic stroke (P = .003), with a 44% higher risk of ischemic
stroke with consumption of more than once per week (HR, 1.44; 95%
CI, 1.12-1.85) compared with consumption of less than once per
month… Among elderly individuals, consumption of tuna or other
broiled or baked fish is associated with lower risk of ischemic
stroke, while intake of fried fish or fish sandwiches is
associated with higher risk.”
|
130
|
|
|
|
Fish
consumption lowers heart disease (CHD) rate
|
Fish
consumption lowers many risk factors for heart disease (HTN,
cholesterol etc.) After controlling for BMI, smoking etc, a lower
heart rate remains statistically significant.
|
131
|
|
|
|
|
The
AHA Scientific Statement of 2003 is available as full free text
and is well-worth reading. It gives a readable summary of very
good evidence, with recommendations:
“…0.3
to 0.5 g/d of EPA+DHA [from fish] and 0.8 to 1.1 g/d of
 -linolenic
acid [e.g., from flax]. Recently, the Food and Nutrition
Board, Institute of Medicine, and The National
Academies, in collaboration with Health Canada, released
the Dietary Reference Intakes for Energy and Macronutrients.107
The Acceptable Macronutrient Distribution Range (AMDR) for
-linolenic
acid is estimated to be 0.6% to 1.2% of energy, or 1.3 to
2.7 g/d on the basis of a 2000-calorie diet. This is -linolenic
acid [e.g., from flax]. Recently, the Food and Nutrition
Board, Institute of Medicine, and The National
Academies, in collaboration with Health Canada, released
the Dietary Reference Intakes for Energy and Macronutrients.107
The Acceptable Macronutrient Distribution Range (AMDR) for
-linolenic
acid is estimated to be 0.6% to 1.2% of energy, or 1.3 to
2.7 g/d on the basis of a 2000-calorie diet. This is
 10
times the current intake of EPA+DHA” 10
times the current intake of EPA+DHA”
“Patients
with CHD should be encouraged to increase their consumption
of EPA and DHA to
1
g/d”
|
132
|
|
|
|
Fish
decreases dementia
|
There
is some evidence that eating fish can reduce the incidence of
dementia (Alzheimer’s disease and the like). One medium-term
(approximately 5 yr. follow-up) study of >1000 French people
found “a significant trend between increasing consumption of
fish or seafood and decreasing incidence of dementia (P for trend
= 0.0091)”
|
133
|
|
|
|
Reduces
risk of prostate cancer
|
A
prospective population study of 47,866 men for 14 yr. found that
“The multivariate [relative risks] of total and advanced
prostate cancer from comparisons of extreme quintiles of the
combination of EPA and DHA were 0.89 (0.77, 1.04) and 0.74 (0.49,
1.08), respectively.”
|
134
|
|
|
|
|
Eating
fish per se (better than fish oil) may reduce prostate cancer
incidence. “We followed 47882 men participating in the Health
Professionals Follow-up Study… Eating fish more than three times
per week was associated with a reduced risk of prostate cancer,
and the strongest association was for metastatic cancer
(multivariate relative risk, 0.56; 95% confidence interval,
0.37-0.86, compared with infrequent consumption, i.e., less than
twice per month).”
|
135
|
|
|
|
Associated
with better intelligence in old age
|
“This
was an observational study of subjects born in 1936 whose mental
ability was tested in 1947 and who were followed up in 2000–2001,
at which time cognition, diet, food supplement use, and risk
factors for vascular disease were assessed… Total erythrocyte
n–3 fatty acids and the ratio of docosahexaenoic acid to
arachidonic acid was associated with better cognitive function in
late life before and after adjustment for childhood IQ.”
|
136
|
|
|
|
Fish
reduces risk of macula degeneration
|
“The
US Twin Study of Age-Related Macular Degeneration comprises
elderly male twins from the National Academy of Sciences-National
Research Council World War II Veteran Twin Registry. To determine
genetic and environmental risk factors for AMD, twins were
surveyed for a prior diagnosis of AMD and underwent an eye
examination, fundus photography, and food frequency and risk
factor questionnaires. This environmental component of the study
includes 681 twins: 222 twins with AMD (intermediate or late
stages) and 459 twins with no maculopathy or early signs. Risk for
AMD according to cigarette smoking and dietary fat intake was
estimated using logistic regression analyses… dietary omega-3
fatty intake was inversely associated with AMD (odds ratio, 0.55;
95% confidence interval, 0.32-0.95) comparing the highest vs
lowest quartile. Reduction in risk of AMD with higher intake of
omega-3 fatty acids was seen primarily among subjects with low
levels (below median) of linoleic acid intake, an omega-6
fatty acid (P trend<.001). The attributable risk percentage
was 32% for smoking and the preventive fraction was 22% for higher
omega-3 intake.”
|
137
|
|
Go
to TOC
Mediterranean
diet
In
essence, a diet rich in olive oil, fish, vegetables, fiber, fruit,
and red wine is healthy.
|
|
Sticking
with the diet significantly reduces risk of heart disease, death
and cancer.
|
“…a
population-based, prospective investigation involving 22,043
adults in Greece who completed an extensive, validated,
food-frequency questionnaire at base line. Adherence to the
traditional Mediterranean diet was assessed by a 10-point
Mediterranean-diet scale that incorporated the salient
characteristics of this diet… A higher degree of adherence to
the Mediterranean diet was associated with a reduction in total
mortality (adjusted hazard ratio for death associated with a
two-point increment in the Mediterranean-diet score, 0.75 …). An
inverse association with greater adherence to this diet was
evident for both death due to coronary heart disease (adjusted
hazard ratio, 0.67 …) and death due to cancer (adjusted hazard
ratio, 0.76 …)…Greater adherence to the traditional
Mediterranean diet is associated with a significant reduction in
total mortality.”
|
138
|
|
|
|
Lessens
rates of all-cause mortality, coronary heart disease,
cardiovascular diseases, and cancer
|
“Healthy
Ageing: a Longitudinal study in Europe (HALE) population,
comprising individuals enrolled in the Survey in Europe on
Nutrition and the Elderly: a Concerned Action (SENECA) and the
Finland, Italy, the Netherlands, Elderly (FINE) studies, includes
1507 apparently healthy men and 832 women, aged 70 to 90 years in
11 European countries. This cohort study was conducted between
1988 and 2000. MAIN OUTCOME MEASURES: Ten-year mortality from all
causes, coronary heart disease, cardiovascular diseases, and
cancer. RESULTS: During follow-up, 935 participants died: 371 from
cardiovascular diseases, 233 from cancer, and 145 from other
causes; for 186, the cause of death was unknown. Adhering to a
Mediterranean diet (hazard ratio [HR], 0.77; 95% confidence
interval [CI], 0.68-0.88), moderate alcohol use (HR, 0.78; 95% CI,
0.67-0.91), physical activity (HR, 0.63; 95% CI, 0.55-0.72), and
nonsmoking (HR, 0.65; 95% CI, 0.57-0.75) were associated with a
lower risk of all-cause mortality (HRs controlled for age, sex,
years of education, body mass index, study, and other factors).
Similar results were observed for mortality from coronary heart
disease, cardiovascular diseases, and cancer. The combination of 4
low risk factors lowered the all-cause mortality rate to 0.35 (95%
CI, 0.28-0.44).”
|
139
|
|
|
|
Lessens
risk of Alzheimer Disease
|
“There
is converging evidence that composite dietary patterns such as the
Mediterranean diet (MeDi) is related to lower risk for
cardiovascular disease, several forms of cancer, and overall
mortality…METHODS: A total of 2,258 community-based nondemented
individuals in New York were prospectively evaluated every 1.5
years. Adherence to the MeDi (zero- to nine-point scale with
higher scores indicating higher adherence) was the main predictor
in models that were adjusted for cohort, age, sex, ethnicity,
education, apolipoprotein E genotype, caloric intake, smoking,
medical comorbidity index, and body mass index. RESULTS: There
were 262 incident AD cases during the course of 4 (+/-3.0; range,
0.2-13.9) years of follow-up…Compared with subjects in the
lowest MeDi tertile, subjects in the middle MeDi tertile had a
hazard ratio of 0.85 (95% confidence interval, 0.63-1.16) and
those at the highest tertile had a hazard ratio of 0.60 (95%
confidence interval, 0.42-0.87) for AD (p for trend = 0.007).
INTERPRETATION: We conclude that higher adherence to the MeDi is
associated with a reduction in risk for AD.”
|
140
|
|
Go
to TOC
Homocysteine
Reduce
the homocysteine level in your blood by taking about 1 mg (1000 mcg)
of folate (folic acid) each day. No, your nor al diet does NOT have
enough folate, even if you eat vegetables and fruit. The Recommended
Daily Allowance (RDA) is 400 mcg and is too little. Common
multivitamins have 400 mcg of folate. Folate works in coordination
with vitamins B6 and B12 to reduce the homocysteine level in your
blood. In fact, folate should be taken with B12 to prevent nerve
damage if you happen to have B12 deficiency (rare in youth). Folate
definitely does the following:
Reduces
the risk for heart attack and other blood vessel disease.
Greatly
reduces the risk for spina bifida if taken during early pregnancy.
In
addition, folate probably also reduces your risk for strokes, certain
cancers (colon and breast), (along with B6 and B12: JAMA 2002-08-29)
recurrence of clogged arteries after an angioplasty, and depression.
Perhaps the best way to reduce homocysteine is caloric
restriction. In one epidemiologic study “Plasma
[homocysteine] level correlated positively with age, body mass index,
and waist-to-hip ratio (P < 0.0001).” (Chan
SJ, Chang CN, Hsu JC, Lee YS, Shen CH. Homocysteine, vitamin B(6),
and lipid in cardiovascular disease. Nutrition. 2002
Jul-Aug;18(7-8):595-8. PMID: 12093437).
Coffee, especially when prepared in the European fashion (very
thick and muddy), may increase homocysteine levels (Urgert
R, van Vliet T, Zock PL, Katan MB. Heavy coffee consumption and
plasma homocysteine: a randomized controlled trial in healthy
volunteers. Am J Clin Nutr. 2000 Nov;72(5):1107-10. PMID: 11063436).
Although regular coffee increases homocysteine levels (“The
increase in homocysteine concentrations 4 h after
consumption of 0.45 L coffee relative to consumption of 3
placebo capsules was 19% (P = 0.0001).” Verhoef
P, Pasman WJ, van Vliet T, Urgert R, Katan MB. Contribution of
caffeine to the homocysteine-raising effect of coffee: a randomized
controlled trial in humans. American Journal of Clinical Nutrition,
Vol. 76, No. 6, 1244-1248, December 2002),
only decaffeinated coffee has been shown to be associated with a
higher rate of heart attack (increased by 25% when compared to
non-drinkers; Sesso
HD, Gaziano JM, Buring JE, Hennekens CH. Coffee and tea intake and
the risk of myocardial infarction. Am J Epidemiol. 1999 Jan
15;149(2):162-7. PMID: 9921961).
Of interest, the best form of vitamin B6 (pyridoxine) may be
pyridoxamine. Pyridoxamine
directly helps to prevent oxidation of lipids
that should also reduce the rate of cardiovascular disease.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Homocysteine
|
Associated
with lower mental function in the elderly
|
“Elevated
plasma tHcy has an independent, graded association with
concurrent cognitive impairment as measured with the
MMSE [Mini-Mental State Examination] in healthy elderly community
dwellers.”
|
141
|
|
|
|
|
“Participants
were from the Veterans Affairs Normative Aging Study. Cognitive
function was assessed with the Mini-Mental State Examination and
on the basis of measures of memory, verbal fluency, and
constructional praxis, which were adapted from the revised
Wechsler Adult Intelligence Scale and the Consortium to Establish
a Registry for Alzheimer's Disease batteries at 2 time points. At
baseline, dietary intakes were assessed with a food-frequency
questionnaire, and blood was drawn for the measurement of B
vitamins and homocysteine. Results: Over a mean 3-y follow-up,
declines in constructional praxis, measured by spatial copying,
were significantly associated with plasma homocysteine, folate,
and vitamins B-6 and B-12 and with the dietary intake of each
vitamin. Folate (plasma and dietary) remained independently
protective against a decline in spatial copying score after
adjustment for other vitamins and for plasma homocysteine. Dietary
folate was also protective against a decline in verbal fluency.
A high homocysteine concentration was associated with a decline in
recall memory. Conclusions: Low B vitamin and high homocysteine
concentrations predict cognitive decline. Spatial copying
measures appear to be most sensitive to these effects in a general
population of aging men.”
|
142
|
|
|
|
Associated
findings
|
More
evidence that folate and B-12 may help: “The unadjusted mean
tHcy was 21.5% ( approximately 1.9 micro mol/L) higher in men than
in women, 11.8% ( approximately 1.1 micro mol/L) higher in
non-Hispanic whites than in Mexican Americans, 42% ( approximately
3.7 micro mol/L) higher in persons aged >/= 70 y than in
persons aged < 30 y, and 10.9% ( approximately 1.0 micro mol/L)
higher in supplement nonusers than in supplement users. The tHcy
concentration was negatively associated with serum folate (P <
0.0001 for trend), RBC folate (P < 0.0001 for trend), and serum
vitamin B-12 (P < 0.0036 for trend)..”
|
143
|
|
|
|
Associated
quite high rates of death from heart disease
|
A 24-year study
of 1368 middle-age women showed that elevated homocysteine levels
(tHcy) were associated with much higher rates of heart attack
(AMI) and death from heart attack. “For the fifth tHcy quintile,
relative risk was 1.86 (95% CI 1.06 to 3.26) for AMI and
5.14 (95% CI 2.22 to 11.92) for death due to AMI.”
|
144
|
|
|
|
Associated
with depression
|
“Those in the
upper tertile for serum tHcy had a more than twofold
(odds ratio: 2.30; 95% CI: 1.35, 3.90; P =
0.002) higher risk of being depressed than did those in
the lowest tertile for serum tHcy. The results remained
significant after adjustment for the month of study, history
of ischemic heart disease, smoking habits, alcohol consumption,
marital status, education, and socioeconomic status in
adulthood (odds ratio: 2.23; 95% CI: 1.30, 3.83;
P = 0.004).”
|
145
|
|
|
|
Reduced
by folate supplements
|
“From the
dose-response curve, the adequate daily dose of folic acid was
estimated to be 392 micro g [mcg], which decreased plasma
homocysteine concentrations 22%.” (note: standard folate pills
and vitamins are at 400 mcg)
|
146
|
|
Go
to TOC
Cholesterol
and triglycerides
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
HDL
cholesterol level
|
Brain
function
Longevity
|
“Plasma
HDL levels correlated significantly with MMSE (r =.32; p <.0001).
Each decrease in plasma HDL tertile (74.9 +/- 2.1, 50.6 +/- 0.5,
and 36.8 +/- 1.0 mg/dl) was associated with a significant decrease
in MMSE (23.4 +/- 1.5, 17.7 +/- 1.8, and 12.4 +/- 1.8; p <.04
for each plasma HDL tertile)… This underscores the protective
effects of increased plasma HDL and its role in maintaining
superior cognition in longevity.”
“Families
of centenarians have high levels of plasma high-density
lipoprotein (HDL) cholesterol”
|
147
|
|
|
|
High
non-HDL cholesterol is bad for the heart
|
“SUMMARY
Non-HDL cholesterol is a potent predictor of cardiovascular risk
among a broad range of individuals with and without cardiovascular
disease and is prognostic over a wide range of follow-up periods.”
|
148
|
|
|
LDL
level
|
Should
be below 100, perhaps below 80
|
Intensive
statin therapy => LDL average = 79 => no progression of
atheroma burden, while those with LDL = 110 => progression. In
other words, this is good evidence that LDL cholesterol should be
very low indeed.
|
149
|
|
|
Cholesterol-lowering
diet
|
Diet
is as good as statin drugs
|
A
cholesterol-lowering diet (“a diet high in plant sterols …,
soy protein…, viscous fibers… and almonds…”) works as well
as statins in a controlled, prospective study. Both interventions
reduced cholesterol and CRP by about 30%.
But
note: phytoestrogens per se from soy & other plant foods do
not seem to lower heart disease risk
|
150
151
152
|
|
|
Statins
|
C
E & β-carotene do NOT help;
statins
do
|
Long
PDF file summarizing the results of a study: vitamins C, E &
β-carotene do not
reduce risk of cancer, cardiovascular disease or any other major
outcome.
On
the other hand, the statins substantially reduce the risk for
vascular events (stroke or heart attack)
|
153
|
|
|
|
Lower
risk of POAG glaucoma
|
“…Longer
duration of statin use was associated with a lower risk of
open-angle glaucoma (P for trend =.04) primarily among subjects
with 24 months or more of use (OR, 0.60) …a protective
association was also observed among those who used nonstatin
cholesterol-lowering agents (OR, 0.59)”
|
154
|
|
Go
to TOC
Whole
grains and bran
Whole
grains (e.g. whole wheat, oat bran) have advantages including
decreased risk of heart disease and improving insulin sensitivity
(vs. diabetes.) One study (Am
J Clin Nutr 2002 Sep;76(3):535-40; PMID: 12197996)
found a 30% reduction in the rate of diabetes in men who ate whole
grain foods, and recommended replacing refined grain foods with whole
grain ones.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Whole
grains
|
Whole
grains are associated with lower mortality and heart disease
|
“Whole-grain
breakfast cereal intake was inversely associated with total and
CVD-specific mortality, independent of age; body mass index;
smoking; alcohol intake; physical activity; history of diabetes,
hypertension, or high cholesterol; and use of multivitamins.
Compared with men who rarely or never consumed whole-grain cereal,
men in the highest category of whole-grain cereal intake (>/= 1
serving/d) had multivariate-estimated relative risks of total and
CVD-specific mortality of 0.83…”
|
155
|
|
|
|
Associated
with lower risk for adult-onset diabetes
|
“An
inverse association between whole-grain intake and the risk of
type 2 diabetes was found. The similar result for cereal fiber
intake suggests that the whole-grain association is due to cereal
fiber or another factor related to cereal fiber intake.”
|
156
|
|
|
|
Good
for bowel health and lower blood glucose
|
“High-fiber
rye and wheat food consumption improved several markers of bowel
and metabolic health relative to that of low-fiber food. Fiber
from rye appears more effective than that from wheat in overall
improvement of biomarkers of bowel health.”
|
157
|
|
|
|
Diabetes
type 2
|
Whole
grains and grain fiber may help prevent diabetes. “An inverse
association between whole-grain intake and the risk of type 2
diabetes was found. The similar result for cereal fiber intake
suggests that the whole-grain association is due to cereal fiber
or another factor related to cereal fiber intake.”
|
158
|
|
|
|
|
“cross-sectional
association between whole- and refined-grain intake,
cardiovascular disease risk factors, prevalence of the metabolic
syndrome, and the incidence of cardiovascular disease mortality in
the same cohort of older adults. DESIGN: The nutritional status of
535 healthy persons aged 60-98 y…The results showed a
significant inverse trend between whole-grain intake and the
metabolic syndrome (P for trend = 0.005) and mortality from
cardiovascular disease (P for trend = 0.04), independent of
demographic, lifestyle, and dietary factors. Fasting glucose
concentrations and body mass index decreased across increasing
quartile categories of whole-grain intake (P for trend = 0.01 and
0.03, respectively), independent of confounders, whereas intake of
refined grain was positively associated with higher fasting
glucose concentrations (P for trend = 0.04) and a higher
prevalence of the metabolic syndrome (P for trend = 0.01).
CONCLUSION: Whole-grain intake is a modifiable dietary risk
factor, and older and young adults should be encouraged to
increase their daily intake to >/=3 servings/d.”
|
159
|
|
|
|
Helps
to prevent obesity
|
“Women
who consumed more whole grains consistently weighed less than did
women who consumed less whole grains (P for trend < 0.0001).
Over 12 y, those with the greatest increase in intake of dietary
fiber gained an average of 1.52 kg less than did those with the
smallest increase in intake of dietary fiber (P for trend <
0.0001) independent of body weight at baseline, age, and changes
in covariate status. Women in the highest quintile of dietary
fiber intake had a 49% lower risk of major weight gain than did
women in the highest quintile (OR = 0.51; 95% CI: 0.39, 0.67; P <
0.0001 for trend).”
|
160
|
|
|
|
|
A
prospective study of whole grain intake and development of
diabetes type II found a 30% reduced risk after adjusting for BMI.
|
161
|
|
|
|
Reduces
periodontitis risk
|
“We
prospectively followed 34 160 male US health professionals aged
40-75 y at the outset. We updated medical and lifestyle
information biennially with questionnaires and diet every 4 y by
using a validated food-frequency questionnaire…Men in the
highest quintile of whole-grain intake were 23% less likely to get
periodontitis than were those in the lowest quintile”
|
162
|
|
|
|
Associated
with lower rate of heart disease
Bran
may be the active part
|
“This
was a prospective cohort study of 42 850 male health professionals
aged 40–75 y at baseline in 1986 who were free from
cardiovascular disease, cancer, and diabetes. Daily whole-grain,
bran, and germ intakes were derived in grams per day from a
detailed semiquantitative dietary questionnaire… The hazard
ratio of CHD in men with the highest intake of added bran was 0.70
(95% CI: 0.60, 0.82) compared with men with no intake of added
bran (P for trend
 0.001).
Added germ was not associated with CHD risk…This study …
suggests that the bran component of whole grains could be a key
factor in this relation.” 0.001).
Added germ was not associated with CHD risk…This study …
suggests that the bran component of whole grains could be a key
factor in this relation.”
|
163
|
|
|
Oat
bran
|
Reduces
cholesterol
|
“The
most significant decreases in total cholesterol (-67.7 +/- 37.2
mg/dl; p < 0.01), low-density lipoprotein cholesterol (-56.3
+/- 35.1 mg/dl; p < 0.01), and apolipoprotein B (-42.4 +/- 34.1
mg/dl; p < 0.01) were found with the combination of the
fat-modified and oat bran enriched food.”
“The
oat bran was incorporated into the daily cooking process (bread
and bread rolls 20-30 g, sauces and desserts 15-20 g), not
detectable for the patients at all.”
|
164
|
|
|
|
|
“34
premenopausal women (age: 22-53 years) were randomly assigned
either to the control group (no supplement) or to the treatment
group, which received 2 oat bran-enriched muffins per day (28
g/day of oat bran) during 4 weeks. RESULTS: Supplementation with
oat bran had a beneficial effect on plasma HDL-C levels. Indeed,
compared to the control group (n = 16), a mean increase in plasma
HDL-C levels of 11.2% was observed in women eating the oat bran
supplement (n = 18) (p = 0.01), whereas the total
cholesterol/HDL-C ratio decreased by 7.0% (p = 0.002).”
|
165
|
|
Go
to TOC
Flax
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Flax
|
Enterolactones
lower the rate of cardiovascular disease and death
Flax
seed intake increases enterolactones
|
“Owing
to its phenolic structure, enterolactone and its plant lignan
precursors, which are converted by intestinal bacteria to
enterolactone, are potential antioxidants… Our data suggest that
a high serum enterolactone level is associated with reduced CHD-
and CVD-related mortality in middle-aged Finnish men. These
results add to the evidence supporting the importance of whole
grain foods, fruits, and vegetables in the prevention of premature
death from CVD.” And "…death decreased linearly across
quartiles of serum enterolactone concentration.”
“The
percentage of flaxseed supplemented test food out of total dietary
intake was 20% of energy… Serum enterolactone concentration was
doubled during flaxseed supplementation.”
|
166
167
|
|
|
|
Flax
lowers cholesterol and triglycerides dramatically, and better than
soy
|
From
a USDA study, where 20% of calories were from ground flax seed:
“In obese rats flaxseed meal had significant cholesterol
lowering effect compared to control rats (41%).” “The marked
hypotriglyceridemic and hypocholesterolemic effects of flaxseed
meal may have important therapeutic implications in patients with
hypertriglyceridemia and hypercholesterolemia…”
|
168
|
|
Go
to TOC
Exercise
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Exercise
|
Cardiovascular
disease
|
“There
is an inverse association between relative intensity of physical
activity (an individual’s perceived level of exertion) and risk
of CHD”
|
169
|
|
|
|
Helps
prevent strokes
|
“Low
cardiorespiratory fitness was comparable with systolic blood
pressure, obesity, alcohol consumption, smoking, and serum
low-density lipoprotein cholesterol level as a risk factor for
stroke.”
|
170
|
|
|
|
Reduces
visceral fat (a risk factor for diabetes)
|
“participants
who exercised at a level equivalent to 17 miles of jogging each
week saw significant declines in visceral fat, subcutaneous
abdominal fat and total abdominal fat”…” participants who
did not exercise had an 8.6 percent increase in visceral fat after
eight months, while those participants who exercised at the
highest amount saw a 8.1 percent decrease in visceral fat.”
|
171
|
|
|
|
Greatly
reduced risk of hypertension
|
“We
prospectively followed 8302 Finnish men and 9139 women aged 25 to
64 years without a history of antihypertensive drug use, coronary
heart disease, stroke, and heart failure at baseline…
Multivariate-adjusted hazards ratios of hypertension associated
with light, moderate, and high physical activity were 1.00, 0.63,
and 0.59 in men (Ptrend<0.001), and 1.00, 0.82, and 0.71 in
women (Ptrend=0.005), respectively. This association persisted
both in subjects who were overweight and in those who were not.
Multivariate-adjusted hazards ratios of hypertension based at
different levels of body mass index (<25, 25 to 29.9, and
>/=30) were 1.00, 1.18, and 1.66 for men (Ptrend<0.001), and
1.00, 1.24, and 1.32 for women (Ptrend=0.007), respectively.”
|
172
|
|
|
|
Helps
keep bones tough and prevent fractures
|
The
primary factor determining bone density and mass is body weight.
However, bone mass does not necessarily prevent fractures: thin
runners have thin but tough bones.
http://www.usc.edu/projects/nexus/faculty/dept-ldsg/wiswell/article.htm
|
|
|
|
|
Reduces
the risk of stroke (CVA) by 27%
|
“a
meta-analysis… [of] 23 studies… For cohort studies, highly
active individuals” (equivalent to running 15-20 min/day, or
exercising 30 min/day) “had a 27% lower risk of stroke
incidence or mortality … than did low-active individuals. We
observed similar results in moderately active individuals compared
with inactive persons (RRs =0.80 …)… We conclude that moderate
and high levels of physical activity are associated with reduced
risk of total, ischemic, and hemorrhagic strokes.”
|
173
|
|
|
|
Increases
longevity by 9% in rats, but not maximum life span
|
“As
in previous studies, wheel running modestly increased average
longevity (approximately 9%), but had no effect on maximal life
span.”
HOWEVER,
from the same author in an earlier paper “the beneficial effects
of food restriction and exercise on survival are not additive or
synergistic.”
Steven
Spindler’s studies of mice show a “squaring of the longevity
curve” with exercise; CR however has a far greater effect.
|
174
175
|
Fig
|
|
|
Reduces
mortality
|
“A
cohort study of vegetarians and health-conscious persons in
Germany was followed-up prospectively for 21 years, including
1,225 vegetarians and 679 health-conscious nonvegetarians.
Standardized mortality ratios compared with the German general
population were calculated for all causes and specific causes…
RESULTS: Standardized mortality ratios for all-cause mortality was
significantly below 100: 59 [95% confidence interval (95% CI),
54-64], predominantly due to a deficit of deaths from circulatory
diseases. Within the cohort, vegetarian compared with
nonvegetarian diet had no effect on overall mortality [rate ratio
(RR), 1.10; 95% CI, 0.89-1.36], whereas moderate and high
physical activity significantly reduced risk of death (RR, 0.62,
0.64), adjusted for age, sex, smoking, alcohol intake, body mass
index, and educational level.”
|
176
|
|
|
|
Too
much exercise may have a long-term detrimental effect
|
“We
conclude that the rate of decline in maximal aerobic capacity
during middle and older age is greater in endurance-trained men
than in their sedentary peers”
|
177
|
|
|
|
Improves
insulin sensitivity
|
A
randomized controlled trial of diet and exercise in 45 obese women
found that “Body weight decreased by approximately 6.5% within
both weight loss groups and was unchanged in the exercise without
weight loss and control groups. In comparison with controls,
cardiorespiratory fitness improved within the exercise groups only
(p < 0.01). Reduction in total, abdominal, and abdominal
subcutaneous fat within the exercise weight loss group was greater
(p < 0.001) than within all other groups… In comparison with
the control group, insulin sensitivity improved within the
exercise weight loss group alone (p < 0.001). DISCUSSION: Daily
exercise without caloric restriction was associated with
substantial reductions in total fat, abdominal fat, visceral fat,
and insulin resistance in women. Exercise without weight loss was
also associated with a substantial reduction in total and
abdominal obesity.”
|
178
|
|
|
|
Reduces
risk for Alzheimer Disease and dementia
|
“Participants
were randomly selected from the survivors of a population-based
cohort previously surveyed in 1972, 1977, 1982, or 1987. 1449
persons (72.5%) age 65-79 years participated in the re-examination
in 1998 (mean follow-up, 21 years). 117 persons had dementia and
76 had AD. Multiple logistic regression methods were used to
analyse the association between leisure-time physical activity and
dementia or AD. FINDINGS: Leisure-time physical activity at
midlife at least twice a week was associated with a reduced risk
of dementia and AD (odds ratio [OR] 0.48 [95% CI 0.25-0.91]
and 0.38 [0.17-0.85], respectively), even after adjustments for
age, sex, education, follow-up time, locomotor disorders, APOE
genotype, vascular disorders, smoking, and alcohol drinking. The
associations were more pronounced among the APOE varepsilon4
carriers. INTERPRETATION: Leisure-time physical activity at
midlife is associated with a decreased risk of dementia and AD
later in life. Regular physical activity may reduce the risk or
delay the onset of dementia and AD, especially among genetically
susceptible individuals.”
|
179
|
|
|
|
|
“1740
persons older than age 65 years without cognitive impairment …were
followed biennially to identify incident dementia… During a mean
follow-up of 6.2 years (SD, 2.0), 158 participants developed
dementia (107 developed Alzheimer disease). The incidence rate
of dementia was 13.0 per 1000 person-years for participants who
exercised 3 or more times per week compared with 19.7 per 1000
person-years for those who exercised fewer than 3 times per week.
The age- and sex-adjusted hazard ratio of dementia was 0.62
(95% CI, 0.44 to 0.86; P = 0.004). The interaction between
exercise and performance-based physical function was statistically
significant (P = 0.013). The risk reduction associated with
exercise was greater in those with lower performance levels.
Similar results were observed in analyses restricted to
participants with incident Alzheimer disease.”
|
180
|
|
|
|
Reduces
risk of macula degeneration (AMD)
|
“The
15-year cumulative incidence of AMD was determined through four
examination phases at five-year intervals of a population-based
study conducted in Beaver Dam, Wisconsin, initiated in 1988-1990
(n=3,874 men and women between ages of 43-86 years)… After
controlling for age, gender, arthritis history, systolic blood
pressure, body mass index, smoking history, and education, persons
with an active lifestyle (defined as regular activity >/= 3
times/week) at baseline were less likely to develop exudative AMD
(odds ratio [OR]= 0.3, 95% confidence interval [CI]=0.1-0.7)
compared to persons without an active lifestyle. After
multivariate adjustment, increased categories of number of
blocks walked per day decreased the risk of exudative AMD (OR=0.7,
95% CI=0.6-0.97). Physical activity was not related to the
incidence of early AMD or pure geographic atrophy. CONCLUSIONS:
These data show a protective effect of physical activity for
incident exudative AMD, independent of body mass index and other
confounders.”
|
181
|
|
|
|
Reduced
risk of colon cancer
|
“We
investigated several aspects of the role of physical activity in
colon and rectal cancer etiology that remain unclear in the
European Prospective Investigation into Nutrition and Cancer. This
cohort of 413,044 men and women had 1,094 cases of colon and 599
cases of rectal cancer diagnosed during an average of 6.4 years of
follow-up. We analyzed baseline data on occupational, household,
and recreational activity to examine associations by type of
activity, tumor subsite, body mass index (BMI), and energy intake.
The multivariate hazard ratio for colon cancer was 0.78 [95%
confidence interval (95% CI), 0.59-1.03] among the most active
participants when compared with the inactive, with evidence of a
dose-response effect (P(trend) = 0.04). For right-sided colon
tumors, the risk was 0.65 (95% CI, 0.43-1.00) in the highest
quartile of activity with evidence of a linear trend (P(trend) =
0.004). Active participants with a BMI under 25 had a risk of 0.63
(95% CI, 0.39-1.01) for colon cancer compared with the inactive.”
|
182
|
|
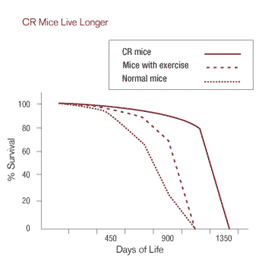
Figure.
Survival curve for mice: normal, on CR diet or given exercise.
Exercise “squares the curve”; CR shifts the curve to the right.
Both help average lifespan, but the effects of CR are much greater.
Go
to TOC
Tea
and coffee
Potential
problems: Caffeine and liquids also give a very small, temporary rise
in blood pressure. If you want less caffeine, "rinse" the
tea bag first for a few seconds with hot water: caffeine dissolves
more easily than the antioxidants, so most of it is washed away. In
addition, to my mind green tea tastes bad. When I drink it (not
often), I add sweetener and spiced tea to make it palatable. Another
problem with tea is oxalic acid that is present in tea just as it is
in spinach. Calcium from milk either in the tea or just before or
after should prevent its absorption.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Caffeine
|
Raises
intraocular pressure (IOP)
|
“In
patients with normotensive glaucoma who drank regular coffee, the
mean +/- SD changes in IOP at 30, 60, and 90 minutes were 0.9 +/-
0.5, 3.6 +/- 1.1, and 2.3 +/- 0.66 mm Hg, respectively; in those
who drank decaffeinated coffee, they were 0.75 +/- 0.36, 0.70 +/-
0.4, and 0.4 +/- 0.6 mm Hg, respectively.”
|
183
|
|
|
|
May
help prevent Alzheimer disease
|
A
retrospective, case control study of 54 AD pts and 54 controls
found that “Using a logistic regression model, caffeine exposure
during this period was found to be significantly inversely
associated with AD (odds ratio=0.40, 95% confidence
interval=0.25-0.67), whereas hypertension, diabetes, stroke, head
trauma, smoking habits, alcohol consumption, non-steroid
anti-inflammatory drugs, vitamin E, gastric disorders, heart
disease, education and family history of dementia were not
statistically significantly associated with AD.”
|
184
|
|
|
Tea
|
Lowers
BP in rats
|
In
rats “systolic and diastolic BP were significantly lower in the
BTP and GTP groups than in the controls… because the amounts of
polyphenols used in this experiment correspond to those in
approximately 1 L of tea, the regular consumption of black and
green tea may also provide some protection against hypertension in
humans.”
|
185
|
|
|
|
Lowers
BP in people
|
“Compared
with nonhabitual tea drinkers, the risk of developing hypertension
decreased by 46% for those who drank 120 to 599 mL/d and was
further reduced by 65% for those who drank 600 mL/d or more after
carefully adjusting for age, sex, socioeconomic status, family
history of hypertension, body mass index, waist-hip ratio,
lifestyle factors (total physical activity, high sodium intake,
cigarette smoking, alcohol consumption, and coffee drinking), and
dietary factors (vegetable, fruit, unrefined grain, fish, milk,
visible-fat food, and deep fried food intake)… CONCLUSION:
Habitual moderate strength green or oolong tea consumption, 120
mL/d or more for 1 year, significantly reduces the risk of
developing hypertension in the Chinese population.”
|
186
|
|
|
|
Benefits
may be eliminated if you drink milk at the same time
|
“Experimental
and clinical studies indicate that tea exerts protection against
cardiovascular diseases…METHODS AND RESULTS: A total of 16
healthy female volunteers consumed either 500 mL of freshly brewed
black tea, black tea with 10% skimmed milk, or boiled water as
control. Flow-mediated dilation (FMD) was measured by
high-resolution vascular ultrasound before and 2 h after
consumption. Black tea significantly improved FMD in humans
compared with water, whereas addition of milk completely blunted
the effects of tea. To support these findings, similar
experiments were performed in isolated rat aortic rings and
endothelial cells. Tea induced vasorelaxation in rat aortic rings
and increased the activity of endothelial nitric oxide synthase by
phosphorylation of the enzyme in endothelial cells. All effects
were completely inhibited by the addition of milk to tea. Of
the various kinds of milk proteins, the caseins accounted for
these inhibiting effects of milk, probably by formation of
complexes with tea catechins. CONCLUSION: Milk counteracts the
favourable health effects of tea on vascular function. This
finding indicates the need for particular awareness in the
interpretation and design of studies comprising nutritional
flavonoids.”
|
187
|
|
|
Green
tea
|
Cancer
|
Green
tea helps prevent cancer
BUT
YOU NEED 10+ CUPS PER DAY!! You can get this much EGCG with
supplement capsules, such as two of AOR’s EGCG MAX capsules per
day.
|
188
189
|
|
|
|
Breast
cancer
|
“Compared
to women who did not drink green tea regularly (i.e., less than
once a month), there was a significant trend of decreasing risk
with increasing amount of green tea intake, adjusted odds ratios
being 1.00, 0.71 (95% confidence interval [CI] 0.51-0.99) and 0.53
(95% CI 0.35-0.78), respectively, in association with no, 0-85.7
and >85.7 ml of green tea per day.”
|
190
|
|
|
Green
tea extract
|
Flavenols
are absorbed as well as from green tea itself
|
“Our
observations suggest that green tea extract supplements
retain the beneficial effects of green and black tea
and may be used in future chemoprevention studies to provide
a large dose of tea polyphenols without the side effects of
caffeine associated with green and black tea beverages.”
|
191
|
|
|
|
Helps
you lose weight
|
“After
a 2-wk diet run-in period, healthy Japanese men were divided into
2 groups with similar BMI and waist circumference distributions. A
12-wk double-blind study was performed in which the subjects
ingested 1 bottle oolong tea/d containing 690 mg catechins (green
tea extract group; n = 17) or 1 bottle oolong tea/d containing 22
mg catechins (control group; n = 18). Results: Body weight, BMI,
waist circumference, body fat mass, and subcutaneous fat area were
significantly lower in the green tea extract group than in the
control group.”
|
192
|
|
|
Coffee
|
High
intake appears associated with heart attack
|
A
case control study showed “…the odds ratios for moderate (<300
mL/d), heavy (300-600 mL/d), and very heavy (>600 mL/d),
consumption, relative to no consumption, were 0.69 (95% CI,
0.50-0.86), 1.56 (95% CI, 1.10-2.34) and 3.10 (95% CI, 1.82-5.26),
respectively, after controlling for the presence of hypertension,
hypercholesterolemia, diabetes mellitus, family history of
premature coronary heart disease, physical activity status,
smoking habits, BMI, alcohol consumption, triglycerides,
consumption of several food items, depression scale score and
education status.”
|
193
|
|
|
|
|
“A
total of 41 836 postmenopausal women aged 55-69 y at baseline were
followed for 15 y. After exclusions for cardiovascular disease,
cancer, diabetes, colitis, and liver cirrhosis at baseline, 27 312
participants remained, resulting in 410 235 person-years of
follow-up and 4265 deaths. The major outcome measure was
disease-specific mortality. RESULTS: … the hazard ratio of death
attributed to cardiovascular disease was 0.76 (95% CI: 0.64, 0.91)
for consumption of 1-3 cups/d, 0.81 (95% CI: 0.66, 0.99) for 4-5
cups/d, and 0.87 (95% CI: 0.69, 1.09) for >/=6 cups/d. The
hazard ratio for death from other inflammatory diseases was 0.72
(95% CI: 0.55, 0.93) for consumption of 1-3 cups/d, 0.67 (95% CI:
0.50, 0.90) for 4-5 cups/d, and 0.68 (95% CI: 0.49, 0.94) for >/=6
cups/d.”
|
194
|
|
|
|
Not
associated with hypertension
|
A
2002 analysis of recent studies of coffee and hypertension found
no association.
|
195
|
|
|
|
|
“Prospective
cohort study conducted in the Nurses' Health Studies (NHSs) I and
II of 155,594 US women free from physician-diagnosed hypertension
followed up over 12 years …no linear association between
caffeine consumption and risk of incident hypertension was
observed after multivariate adjustment”
|
196
|
|
|
|
Homocysteine
|
“The
increase in homocysteine concentrations 4 h after consumption of
[two cups of] coffee relative to consumption of 3 placebo capsules
was 19% (P = 0.0001). Caffeine treatment had a much weaker acute
effect on homocysteine (4%; P = 0.09). Effects of caffeine were
stronger in women than in men, but the effects of coffee did not
differ significantly between men and women. CONCLUSIONS: Caffeine
is partly responsible for the homocysteine-raising effect of
coffee. Coffee, but not caffeine, affects homocysteine metabolism
within hours after intake, although the effect is still
substantial after an overnight fast.”
|
197
|
|
|
|
May
protect against stroke and all-cause mortality
|
A
Japanese study of “2,855 men and women aged 40-79 years in 1989,
and during the subsequent 9.9 years of follow-up. Using the Cox
regression model to adjust for potential confounding factors, we
calculated the multivariate hazard ratios of death from all causes
separately for men and women. The multivariate hazard ratio of
mortality for men who consumed two or more cups of coffee per day,
compared with those who consumed less than half a cup per day, was
0.43 (95% confidence interval, 0.30-0.63), and the ratio for those
who consumed half to one cup of coffee per day was 0.70 (95%
confidence interval, 0.52-0.94).”
|
198
|
|
|
|
Appears
to protect against diabetes type 2
Drinking
6 cups/day reduces risk by about 30%
|
A
large, prospective 18-year Swedish follow-up study showed that
“Associated hazard ratios, after adjustment for age, smoking,
low physical activity, education and body mass index were 0.55
(0.32-0.95), 0.39 (0.20-0.77) and 0.48 (0.22-1.06) for daily
consumption of three to four, five to six and seven cups or more,
respectively, with a consumption of less than two per day as
reference.”
A
large, prospective Dutch study showed that “After adjustment for
potential confounders, individuals who drank at least seven cups
of coffee a day were 0.50 (95% CI 0.35-0.72, p=0.0002) times as
likely as those who drank two cups or fewer a day to develop type
2 diabetes.”
This
was also found in the Nurses’ Health Study: “The authors found
an inverse association between coffee intake and type 2 diabetes
after adjustment for age, body mass index, and other risk factors.
The multivariate relative risks for diabetes according to regular
coffee consumption categories (0, <1, 1 to 3, 4 to 5, or >
or =6 cups per day) in men were 1.00, 0.98, 0.93, 0.71, and 0.46
(95% CI, 0.26 to 0.82; P = 0.007 for trend), respectively. The
corresponding multivariate relative risks in women were 1.00,
1.16, 0.99, 0.70, and 0.71 (CI, 0.56 to 0.89; P < 0.001 for
trend), respectively. For decaffeinated coffee, the multivariate
relative risks comparing persons who drank 4 cups or more per day
with nondrinkers were 0.74 (CI, 0.48 to 1.12) for men and 0.85
(CI, 0.61 to 1.17) for women. Total caffeine intake from coffee
and other sources was associated with a statistically
significantly lower risk for diabetes in both men and women.
CONCLUSIONS: These data suggest that long-term coffee consumption
is associated with a statistically significantly lower risk for
type 2 diabetes.”
And
again in a study from Finland in JAMA: “After adjustment for
confounding factors (age, study year, body mass index, systolic
blood pressure, education, occupational, commuting and
leisure-time physical activity, alcohol and tea consumption, and
smoking), the HRs [Hazard Ratios] of DM associated with the amount
of coffee consumed daily (0-2, 3-4, 5-6, 7-9, > or =10 cups)
were 1.00, 0.71 … 0.39 … 0.39 … and 0.21 …(P for
trend<.001) in women, and 1.00, 0.73 …0.70 … 0.67 … and
0.45 … (P for trend =.12) in men, respectively. In both sexes
combined, the multivariate-adjusted inverse association was
significant (P for trend <.001) and persisted when stratified
by younger and older than 50 years; smokers and never smokers;
healthy weight, overweight, and obese participants; alcohol
drinker and nondrinker; and participants drinking filtered and
nonfiltered coffee. CONCLUSION: Coffee drinking has a graded
inverse association with the risk of type 2 DM”
A
large review in JAMA (2005) of 9 cohort studies found that “The
[Relative Risk] of type 2 diabetes was 0.65 (95% confidence
interval [CI], 0.54-0.78) for the highest (>or=6 or >or=7
cups per day) and 0.72 (95% CI, 0.62-0.83) for the second highest
(4-6 cups per day) category of coffee consumption compared with
the lowest consumption category (0 or <or=2 cups per day).”
|
199
200
201
202
203
|
|
|
|
Associated
with lower risk of breast cancer
|
“A
hospital-based, case-control study … 1932 cases with primary,
incident breast cancer and 1895 hospital controls with
nonneoplastic conditions… Among premenopausal women, consumption
of regular coffee was associated with linear declines in breast
cancer risk (P for trend = 0.03); consumers of >/=4 cups/d
experienced a 40% risk reduction (odds ratio = 0.62, 95% CI
0.39-0.98).”
|
204
|
|
|
Carbonated
soft drinks
|
Associated
with lower risk of esophageal cancer
|
“we
examined CSD [Carbonated soft drinks] as a risk factor for
esophageal and gastric cancers in a U.S. multicenter,
population-based case-control study. Associations between CSD
intake and risk were estimated by adjusted odds ratios (ORs),
comparing the highest versus lowest quartiles of intake. All
statistical tests were two-sided. Contrary to the proposed
hypothesis, CSD consumption was inversely associated with
esophageal adenocarcinoma risk (highest versus lowest quartiles,
OR = 0.47, 95% confidence interval = 0.29 to 0.76; Ptrend = .005)”
|
205
|
|
Go
to TOC
Antioxidants
Free
radicals. These are intermediate chemical reactants, a by-product of
living and processing the food we eat! They are very reactive and
cause slow, continuous damage to cells and tissues all over the body,
and may account for part of the aging process in the brain. As we
age, free radicals are produced in greater amounts. The body has
several systems to neutralize these reactive chemicals, especially
bilirubin “bilirubin is a major physiologic antioxidant
cytoprotectant” (Baranano
DE, Rao M, Ferris CD, Snyder SH. Biliverdin reductase: a major
physiologic cytoprotectant. Proc Natl Acad Sci U S A. 2002 Dec
10;99(25):16093-8. PMID: 12456881)),
glutathione and uric acid. Mutant lab animals with defects in these
systems age and die rapidly. Fortunately there are a few things you
can do to reduce the effect of free radicals.
First, you
can reduce the production of free radicals by eating less (see the
section on caloric
restriction). This is by far the
cheapest and most effective (in theory) approach, with the fewest
side effects! In fact fasting for a day temporarily reduces the
level of free radical damage by a very large amount, about 1/3.
Second, you can reduce the risk of damage from free radicals by
getting a portion of your calories monounsaturated fat (MUFA) from
nuts, and reducing polyunsaturated fats such as corn oil and other
sources rich in omega-6 fats.
Third, you can get a variety
(Int
J Epidemiol 2002 Aug;31(4):847-54) of
antioxidants from vegetables (especially spinach, broccoli and
related vegetables), nuts and fruits (especially blueberries,
strawberries, raspberries [shown
to reduce risk of cancer in the lab],
prunes and purple grape juice), green or black tea, and other things.
Antioxidant-rich
blueberries, spinach and strawberries have been shown to improve
brain function in rats.
Blueberries have also been shown to be equal to CR in protecting
brain function in rats (Mech
Ageing Dev 1999 Nov;111(2-3):141-54; PMID: 10656533).
On the other hand, antioxidants in general have NOT been shown to
reduce the risk of coronary heart disease (Am
J Clin Nutr 2002 Feb;75(2):191-212; PMID: 11815309).
Tea and flavenoids, however, HAVE recently been shown to be
associated with a very large drop in heart disease – up to 70%! (Am
J Clin Nutr 2002 May;75(5):880-6; PMID: 11976162)
I think it is best not to place too much emphasis on antioxidants.
They probably help up to a point, but are secondary and perhaps not
worth fretting about too much if you eat lots of fruit and vegetables
and drink tea. N.b., simultaneous intake of milk may eliminate the
antioxidant qualities of tea (Int
J Food Sci Nutr 2000 Sep;51(5):309-15; PMID: 11103296).
Note: studies on the effect of antioxidants in lifespan of lab
mammals show NO EFFECT, or even a detriment (for coenzyme Q-10, a
popular supplement).
Caveat: tea from tea bags has a
substantial amount of fluoride, in part from the fluoridated
pesticides used on tea leaves (the same applies to other fruit and
vegetables, such as grapes). Fluoride gets permanently deposited in
bone. It is a highly toxic poison (read the label on your
toothpaste!) It increases the density of bone but actually weakens it
(perhaps making it more brittle), making it prone to fractures. One
study showed a small but significant increase in hip fractures in
areas where there was a moderate or high level of fluoride in the
water (J
Bone Miner Res 2001 May;16(5):932-9; PMID: 11341339).
You need fluoride in toothpaste to harden your teeth to tooth decay,
but I think it is best to avoid excess fluoride ingestion if you plan
to live long! Fortunately, the tea extract in commonly available
capsules is said to have little or no fluoride.
In a
study of death rates related to diet and other factors (Epidemiology
1997 Mar;8(2):168-74; PMID: 9229209):
the mortality hazard ratios with ... increasing [amounts of]... nuts
(1.00, 0.60, 0.56), fruits (1.00, 0.38, 0.57), and green salads
(1.00, 0.54, 0.65). Thus the often heard exhortation to eat more
fruits, vegetables & nuts. All of these foods have antioxidants
of various kinds.
Another study from rural Japan found that
people with the highest levels of serum antioxidants (carotenes,
lycopene, beta-cryptoxanthin, canthaxanthin, zeaxanthin, lutein; NOT
tocopherols (vit E) or retinol (vit A)) had the lowest levels of
cancer and all-cause mortality (Int
J Vitam Nutr Res 2002 Jul;72(4):237-50; PMID: 12214561).
A Finnish study found that high lycopene levels were associated
with intima-media thickening of the common carotid artery,
that has been shown to predict coronary events (Rissanen
TH, Voutilainen S, Nyyssönen K, Salonen R, Kaplan GA and Salonen
JT. Serum lycopene concentrations and carotid atherosclerosis: the
Kuopio Ischaemic Heart Disease Risk Factor Study. American Journal of
Clinical Nutrition, Vol. 77, No. 1, 133-138, January 2003),
thus lycopene may help prevent heart disease and stroke.
Lutein & zeaxanthin have also been shown to be at low levels in
the maculae (the central part of the retina) of patients with macula
degeneration (AMD). In AMD patients who took high-dose lutein
supplements, these levels returned to normal (Bernstein
PS, Zhao DY, Wintch SW, Ermakov IV, McClane RW, Gellermann W.
Resonance Raman measurement of macular carotenoids in normal subjects
and in age-related macular degeneration patients. Ophthalmology. 2002
Oct;109(10):1780-7. PMID: 12359594).
There is also evidence that people with the highest food intake of
lutein and zeaxanthin (e.g. spinach & kale) have the lowest rate
of AMD (Seddon
JM, Ajani UA, Sperduto RD, Hiller R, Blair N, Burton TC, Farber MD,
Gragoudas ES, Haller J, Miller DT, et al. Dietary carotenoids,
vitamins A, C, and E, and advanced age-related macular degeneration.
Eye Disease Case-Control Study Group. JAMA. 1994 Nov
9;272(18):1413-20. PMID: 7933422). What
is not yet proven is whether these supplements can prevent, slow or
reverse AMD. This is being studied: a pilot study states that
“results suggest that increasing the level of retinal
antioxidants might influence macular function early in the disease
process, as well as in normal aging.” (Falsini
B, Piccardi M, Iarossi G, Fadda A, Merendino E, Valentini P.
Influence of short-term antioxidant supplementation on macular
function in age-related maculopathy: a pilot study including
electrophysiologic assessment. Ophthalmology. 2003 Jan;110(1):51-60;
discussion 61. PMID: 12511345)
-
|
Food
|
Lutein
& zeaxanthin per serving (mg)
|
|
Kale
|
26
|
|
Collard
greens
|
15
|
|
Spinach,
fresh cooked
|
13
|
|
Turnip
greens
|
12
|
|
Broccoli
|
4
|
|
Spinach,
frozen cooked
|
4
|
|
Squash
|
3
|
|
Peas
|
2
|
|
Sweet
corn
|
1.5
|
|
Lettuce
|
1.5
|
|
Brussels
sprouts
|
1
|
The
best research seems to show that antioxidants of most (if not all)
kinds can prolong the mean lifespan of lab animals but NOT the
maximum lifespan (Barja
G. Rate of generation of oxidative stress-related damage and animal
longevity. Free Radic Biol Med. 2002 Nov 1;33(9):1167-1172. PMID:
12398924). This implies that antioxidants
help reduce the risk of certain diseases, but do not slow the aging
process itself. To do both, practice caloric restriction.
Here
is a useful summary using the antioxidant
analysis called ORAC. The
antioxidant foods on top of the list have the most effect ON THIS
ARTIFICIAL TEST OF UNCERTAIN VALUE per calorie. In vivo, spinach
comes out on top of several tested (see the USDA article Cans
Foods Forestall Aging?),
but there are many different types of anti-oxidants, and it may be
best to eat a variety (Int
J Epidemiol 2002 Aug;31(4):847-54) of
them every day. The list below is of many but not by any means all
anti-oxidant food sources. ORAC/Cal
– the most “bang for the buck”:
-
|
Food
sorted by ORAC per calorie
|
ORAC/cal
|
ORAC/100
gm
|
|
Clove
oil (Syzigium aromaticum)
|
11,985
|
10,786,875
|
|
Wolfberries
|
633
|
25,300
|
|
Thyme
oil (Thymus vulgaris)
|
177
|
159,590
|
|
Oregano
oil (Origanum compactum)
|
170
|
153,007
|
|
Mountain
Savory oil (Satureja montana)
|
126
|
113,071
|
|
Spinach
|
57
|
1,260
|
|
Strawberries
|
51
|
1,540
|
|
Blueberries
|
43
|
2,400
|
|
Blackberries
|
39
|
2,036
|
|
Kale
|
35
|
1,770
|
|
Broccoli
Flowers
|
32
|
890
|
|
Red
bell pepper
|
26
|
710
|
|
Raspberries
|
25
|
1,220
|
|
Prunes
|
24
|
5,770
|
|
Brussels
sprouts
|
23
|
980
|
|
Beets
|
20
|
840
|
|
Plums
|
17
|
949
|
|
Oranges
|
16
|
750
|
|
Eggplant
|
15
|
390
|
|
Grapefruit,
pink
|
15
|
483
|
|
Cherries
|
13
|
670
|
|
Onion
|
12
|
450
|
|
Red
grapes
|
10
|
739
|
|
Kiwi
fruit
|
10
|
602
|
|
Raisins
|
9
|
2,830
|
|
Corn
|
5
|
400
|
Food
ORAC/ ORAC/
Cal
g
----------------------------------------
Cauliflower
15.6 3.9
Cabbage
14 3.5
Garlic
13.1 19.5
Onion
11.8 4.5
Cantaloupe
8.6 3
White
grape 6.7 4.5
Apricot
4.2 2
Sweet
potato (yams) 3 3.5
Interestingly,
red
& violet onions have about three times as much of the antioxidant
quercetin as common onions. This
finding matches the correlation between color and antioxidants found
in colored vegetables.
Recent data also show that the ORAC
and FRAP (ferric reducing antioxidant capacity) values of vegetable
are not only dependent on species, but also highly dependent on
geographical origin and harvest time (J
Agric Food Chem 2002 May 22;50(11):3122-8; PMID: 12009973).
Remarkably,
some essential oils (spice oils) have far more antioxidant power on
ORAC assays than fruits and vegetables. Cloves come out on top, with
two drops of oil equivalent to 2.5 cups of blueberries. Clove
oil (eugenol) is used as a local anesthetic by dentists; ground
cloves contain 15% eugenol and are tasty in some foods.
I like to put them on thawed frozen blackberries & blueberries!
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Antioxidants
|
Link
to a table
|
USDA
web site with list of flavenoid content of many foods, such as
berries, tea, etc. Of interest is that green tea has much more of
many flavenoids than prepared tea powders etc.
|
206
|
|
|
|
ORAC
is NOT the best measure of effect
|
Well
thought out quote from Michael Rae: “I've often ranted about
people citing ORAC and other test-tube measures of alleged
antioxidant capacity to draw conclusions about the health value of
various foods. In brief, the 2 biggest issues are that (1) because
different kinds of antioxidants quench different kinds of
radicals, any existing measure of 'antioxidant capacity' can only
represent a narrow range of a given substance's antioxidant
effects; [ORAC only measures phenolic antioxidant donor capacity.
So for example, gamma tocopherol has a much lower ORAC than alpha,
which against SOME ROS (say, hydroxyl radical) is an accurate
assay of their relative potency -- but gamma is much more powerful
against peroxynitrite and other nitrogen-based "free
radicals," and ORAC totally misses this. It also can't
account for the compartmentalization & distribution of
specific antioxidant molecules: whether they work in the fluids of
the body or in the membranes, whether they can be transported
actively into various key compartments or are only able to
dissolve & diffuse, etc]; and (2) because of different
absorption & metabolism of various antioxidant compounds (esp
phenolics [which are the antioxidants whose value is always put in
the most impressive light by ORAC and in which fruit is rich]),
something can have gangbuster antioxidant activity in a test tube
& be irrelevant in vivo because the compound in the food just
doesn't get into your system. (There is also the whole question of
whether something's simply being an antioxidant actually
constitutes a health benefit).”
|
207
|
|
|
|
Which
flavenoids matter for heart disease?
|
A
case-control study from Greece found that only “Flavan-3-ols,
which are largely found in wine and tea, are inversely associated
with, and may be protective against, coronary heart disease.”
Also, “an increase of about 21 mg per day corresponding to a 24%
decrease in CHD risk. The inverse association between flavan-3-ols
and CHD risk was largely accounted for by the intake of wine and
to a lesser extent tea.” Flavan-3-ols, specifically the
catechins, are abundant in ripe fruits, leaves, tea and red wine.
|
208
|
|
|
|
Numerous
antioxidant data
|
FDA
(PDF-format) document lists a large number of antioxidant
compounds and activity in foods. Note: this does NOT necessarily
correspond with benefit to humans.
|
209
|
|
|
|
Do
NOT affect lifespan
|
Two
of the most touted antioxidants do not improve lifespan of mice.
“…alpha-lipoic acid or coenzyme Q(10)… had no impact on
longevity or tumor patterns compared with control mice fed the
same number of calories, whereas [caloric restriction] increased
maximum life span by 13% (p <.0001) and reduced tumor
incidence.”
n.b.,
this has been confirmed elsewhere with these and other
supplements.
|
210
|
|
|
Dietary
beta carotene, vitamin C & E, and zinc
|
Linked
to slightly lower macula degeneration rates
|
“Recently,
high-dose supplementation with beta carotene, vitamins C and E,
and zinc was shown to slow the progression of AMD. OBJECTIVE: To
investigate whether regular dietary intake of antioxidants
is associated with a lower risk of incident AMD. DESIGN: Dietary
intake was assessed at baseline in the Rotterdam Study (1990-1993)
using a semiquantitative food frequency questionnaire. Incident
AMD until final follow-up in 2004 was determined by grading fundus
color transparencies in a masked way according to the
International Classification and Grading System. SETTING:
Population-based cohort of all inhabitants aged 55 years or older
in a middle-class suburb of Rotterdam, the Netherlands.
PARTICIPANTS: Of 5836 persons at risk of AMD at baseline, 4765 had
reliable dietary data and 4170 participated in the follow-up. MAIN
OUTCOME MEASURE: Incident AMD, defined as soft distinct drusen
with pigment alterations, indistinct or reticular drusen,
geographic atrophy, or choroidal neovascularization. RESULTS:
Incident AMD occurred in 560 participants after a mean follow-up
of 8.0 years (range, 0.3-13.9 years). Dietary intake of both
vitamin E and zinc was inversely associated with incident AMD. The
hazard ratio (HR) per standard deviation increase of intake for
vitamin E was 0.92 (95% confidence interval [CI], 0.84-1.00) and
for zinc was 0.91 (95% CI, 0.83-0.98). An above-median intake of
all 4 nutrients, beta carotene, vitamin C, vitamin E, and zinc,
was associated with a 35% reduced risk (HR, 0.65; 95% CI,
0.46-0.92) of AMD. Exclusion of supplement users did not affect
the results. CONCLUSION: In this study, a high dietary intake of
beta carotene, vitamins C and E, and zinc was associated with a
substantially reduced risk of AMD in elderly persons.”
|
211
|
|
|
|
|
A
popularized summary website of AMD macula degeneration risk
factors.
|
212
|
|
Go
to TOC
Vegetables
and fruits
DO
NOT do the Atkins diet! It is bad for you.
I
have heard that the “South Beach Diet” advocates avoiding
unhealthy types of fats etc., thus it may be a variant that is quite
good for you. I do not know!
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
How
to eat
|
Eat
with oil for absorption of carotenoids
|
No
oil => no absorption!
|
213
|
|
|
Vegetables
|
High
intake is associated with longer lifespan
|
A
30-year follow-up study of 1536 Italian males showed a 1-year gain
in lifespan of non-smokers (2 years in smokers).
|
214
|
|
|
|
Associated
with a reduced rate of cognitive decline
|
“a
prospective cohort study of 3,718 participants, aged 65 years and
older of the Chicago Health and Aging Project. Participants
completed a food frequency questionnaire and were administered at
least two of three cognitive assessments at baseline, 3-year, and
6-year follow-ups. … The mean cognitive score at baseline for
the analyzed cohort was 0.18 (range: -3.5 to 1.6), and the overall
mean change in score per year was a decline of 0.04 standardized
units. In mixed effects models adjusted for age, sex, race, and
education, compared with the rate of cognitive decline among
persons in the lowest quintile of vegetable intake (median of 0.9
servings/day), the rate for persons in the fourth quintile
(median, 2.8 servings/day) was slower by 0.019 standardized units
per year (p = 0.01), a 40% decrease, and by 0.018
standardized units per year (p = 0.02) for the fifth quintile
(median, 4.1 servings/day), or a 38% decrease in rates. The
association remained significant (p for linear trend = 0.02) with
further control of cardiovascular-related conditions and risk
factors. Fruit consumption was not associated with cognitive
change. CONCLUSION: High vegetable but not fruit consumption
may be associated with slower rate of cognitive decline with older
age.”
|
215
|
|
|
|
Reduces
kidney stones from uric acid
|
Uric
acid (think gout, kidney stones) comes from purine metabolism;
purine comes from DNA in cells, most concentrated in meat. Thus
meat => these problems. “The ingestion of the vegetarian diet
… led to a further significant reduction in the risk of uric
acid crystallization by 93% compared to [the Western type diet].”
|
216
|
|
|
|
|
Some
people are sensitive to the bitter taste of some vegetables. It
turns out that the gene (TAS2R38) that is associated with being a
“PTC taster” (phenylthiocarbamide) correlates well with
avoiding vegetables in children! PTC strips is the common test
often used in high school genetics.
|
217
|
|
|
Fruit
and vegetables
|
May
help prevent dementia
|
Fruit
(blueberries and strawberries) and vegetables (spinach) may help
prevent neuronal aging (dementia), perhaps via anti-oxidant
properties.
|
218
|
|
|
|
|
From
Reuters: [Researchers] “divided the dogs into four groups that
got either standard care; a diet supplemented with tomatoes,
carrot granules, citrus pulp, spinach flakes and supplements;
standard care plus extra exercise and play; or the special diet
and the special play and exercise regime. A second set of 17 dogs
aged 1 to 3 got either a standard or fortified diet. Tests
included having to find a hidden treat. The older dogs clearly
benefited from the special diet and the special exercise program,
the researchers said. All 12 of the older beagles that got a
supplemented diet and exercise could solve a difficult problem,
compared to eight of 10 dogs that got the enriched diet alone and
two of eight dogs that got no special treatment.”
|
219
|
|
|
|
Lower
LDL levels
|
“Fruit
and vegetable consumption was inversely related to LDL: in
the categories 0–1.9, 2.0–2.9, 3.0–3.9, and
 4
servings/d, multivariate-adjusted mean (95% CI) LDL
concentrations were 3.36 (3.28, 3.44), 3.35 (3.27, 3.43),
3.26 (3.17, 3.35), and 3.17 (3.09, 3.25) mmol/L,
respectively, for men (P for trend < 0.0001)
and 3.35 (3.26, 3.44), 3.22 (3.14, 3.30), 3.21 (3.13,
3.29), and 3.11 (3.04, 3.18), respectively, for women
(P for trend < 0.0001).” 4
servings/d, multivariate-adjusted mean (95% CI) LDL
concentrations were 3.36 (3.28, 3.44), 3.35 (3.27, 3.43),
3.26 (3.17, 3.35), and 3.17 (3.09, 3.25) mmol/L,
respectively, for men (P for trend < 0.0001)
and 3.35 (3.26, 3.44), 3.22 (3.14, 3.30), 3.21 (3.13,
3.29), and 3.11 (3.04, 3.18), respectively, for women
(P for trend < 0.0001).”
|
220
|
|
|
|
Improve
bone health in girls
|
“High
fruit and vegetable intakes have beneficial effects on
the bone area of the radius and whole body in early pubertal
girls.”
|
221
|
|
|
|
There
is only a modest effect on chronic disease
|
“Of
the food groups analyzed, green leafy vegetable intake showed the
strongest inverse association with major chronic disease and
cardiovascular disease. For an increment of one serving per day of
green leafy vegetables, relative risks were 0.95 (95% CI = 0.92 to
0.99) for major chronic disease and 0.89 (95% CI = 0.83 to 0.96)
for cardiovascular disease. CONCLUSIONS: Increased fruit and
vegetable consumption was associated with a modest although not
statistically significant reduction in the development of major
chronic disease. The benefits appeared to be primarily for
cardiovascular disease and not for cancer.”
My
thoughts: there still may be some fruit and vegetables that are
good at preventing certain types of cancer.
|
222
|
|
|
|
|
“Current
evidence supports the inclusion of whole grains, fruits and
vegetables, and lean sources of animal proteins including low-fat
dairy products in dietary therapies for insulin resistance. Those
who wish to follow a low-carbohydrate diet should be encouraged to
follow a new menu low in fat, and with most of the protein derived
from plant sources.”
|
223
|
|
|
|
Lower
C-Reactive Protein (CRP)
|
“…high
intake (8 servings/d) of vegetables and fruit significantly
increased total carotenoid concentrations in plasma … C-reactive
protein was significantly reduced at week 8 in the subjects who
consumed 8 servings/d of vegetables and fruit compared with those
who consumed 2 servings/d.”
|
224
|
|
|
|
Reduced
risk of stroke
|
A
meta-analysis of prospective studies “including 90,513 men,
141,536 women, and 2,955 strokes” showed “The risk of
stroke was decreased by 11%... for each additional portion per day
of fruit, by 5% ... for fruit and vegetables, and by 3% ... for
vegetables.”
|
225
|
|
|
|
|
A
meta-analysis in Lancet “Eight studies, consisting of nine
independent cohorts, met the inclusion criteria. These groups
included 257,551 individuals (4917 stroke events) with an average
follow-up of 13 years. Compared with individuals who had less than
three servings of fruit and vegetables per day, the pooled
relative risk of stroke was 0.89 (95% CI 0.83-0.97) for those with
three to five servings per day, and 0.74 (0.69-0.79) for those
with more than five servings per day. Subgroup analyses showed
that fruit and vegetables had a significant protective effect on
both ischaemic and haemorrhagic stroke…Our results provide
strong support for the recommendations to consume more than five
servings of fruit and vegetables per day, which is likely to cause
a major reduction in strokes.”
|
226
|
|
|
|
Associated
with reduced risk of oral cancer
|
Meta-analysis:
“A comprehensive, systematic bibliographic search of medical
literature published up to September 2005 was conducted to
identify relevant studies. Separate meta-analyses were conducted
for fruit and vegetable consumption. The effect of portion or
daily intake of fruit or vegetables on the risk of oral cancer was
calculated. A multivariate meta-regression analysis was performed
to explore heterogeneity. This multivariate meta-regression
analysis examined the effect of quality score, the type of cancers
included, citrus fruit and green vegetable consumption, and the
time interval for dietary recall of the studies on the role of
fruit or vegetable consumption in the risk of oral cancer. The
presence of publication bias was assessed with a funnel plot for
asymmetry. RESULTS: Sixteen studies (15 case-control studies and 1
cohort study) met the inclusion criteria and were included in the
meta-analysis. The combined adjusted odds ratio (OR) estimates
showed that each portion of fruit consumed per day significantly
reduced the risk of oral cancer by 49% (OR: 0.51; 95% CI:
0.40, 0.65). For vegetable consumption, the meta-analysis
showed a significant reduction in the overall risk of oral cancer
of 50% (OR: 0.50; 95% CI: 0.38, 0.65)…The consumption of
fruit and vegetables is associated with a reduced risk of oral
cancer.”
|
227
|
|
|
|
Reduces
risk of coronary heart disease (CHD)
|
A
meta-analysis of studies found “The pooled RRs were calculated
for each additional portion of fruit and/or vegetables consumed
per day, and the linearity of the associations were examined. Nine
studies were eligible for inclusion in the meta-analysis that
consisted of 91,379 men, 129,701 women, and 5,007 CHD events. The
risk of CHD was decreased by 4% …for each additional portion per
day of fruit and vegetable intake and by 7% … for fruit
intake…This meta-analysis of cohort studies shows that fruit
and vegetable consumption is inversely associated with the risk of
CHD. The causal mechanism of this association, however, remains to
be demonstrated.”
|
228
|
|
|
Broccoli
& other crucifers (Brussels sprouts, cauliflower, etc.)
|
Helps
prevent certain cancer
|
Broccoli
and related vegetables have been shown to reduce the rate of
certain cancers. This is NOT because of antioxidant activity;
instead they contain certain molecules (glucosinolate,
isothiocyanates (ITC) and indoles) that induce an increase in the
body’s production of what is called “Phase 2 enzymes”. These
enzymes detoxify certain carcinogens by causing an increase in
glutathione-S-transferase (GST) activity. The response to these
vegetables appears to be dependent on your genes. The most potent
vegetable inducer of this is broccoli sprouts, easily grown at
home (I do).
|
229
|
|
|
|
Helps
prevent stomach ulcers and cancers
|
In
addition, the nutrient sulphorophane is found in broccoli and
broccoli sprouts: it has been shown to kill Heliobacter pylori, a
common pathogenic bacterium that causes stomach cancer and stomach
ulcers.
|
230
|
|
|
|
Acidic
salad dressing increases; long cooking eliminates sulforaphane
|
“Broccoli
contains sulforaphane, an anticarcinogen with multiple
chemoprotective effects. Upon disruption of broccoli tissue,
bioactive sulforaphane … are … formed by myrosinase-dependent
hydrolysis of glucoraphanin, a glucosinolate precursor. Since
production of these compounds occurs only after the plant tissue
is disrupted” “A pH of 3.5, typical of many salad dressings,
significantly increased sulforaphane from 17% to 41% of detected
glucoraphanin hydrolysis products, at the expense of sulforaphane
nitrile. …Steam blanching longer than 1 minute significantly
decreased production of [sulforaphane + sulforaphane nitrile] to
<3% of pre-steamed, indicating inactivation of myrosinase.”
|
231
|
|
|
|
|
“We conclude
that a diet containing phase 2 protein inducers” [e.g.
broccoli sprouts] “also reduces the risk of developing
cardiovascular problems of hypertension and atherosclerosis.”
|
232
|
|
|
|
Slow
mental aging
|
“We
prospectively examined fruit and vegetable intake in relation to
cognitive function and decline among aging women. Participants
were followed from in 1976 with biennial questionnaires, and food
frequency questionnaires were administered in 1984, 1986, and
every 4 years thereafter. From 1995 to 2001, we administered, by
telephone, six cognitive tests measuring general cognition, verbal
memory, category fluency, and working memory. We repeated
assessments two years later for 13,388 women (>90%
follow-up)…Fruits were not associated with cognition or
cognitive decline. However, total vegetable intake was
significantly associated with less decline. Specifically, on a
global score combining all tests, women in the highest quintile of
cruciferous vegetables declined slower (by 0.04 unit; 95%
confidence interval, 0.003, 0.07; p trend = 0.1) compared with the
lowest quintile. Women consuming the most green leafy
vegetables also experienced slower decline than women
consuming the least amount (by 0.05 unit; 95% confidence interval,
0.02, 0.09; p trend < 0.001). These mean differences were
equivalent to those observed for women about 1 to 2 years apart in
age.”
|
233
|
|
|
Garlic
& Onions
|
May
help prevent prostate cancer
|
“Men in the
highest of three intake categories of total allium vegetables
[garlic, onions etc.] (>10.0 g/day) had a statistically
significantly lower risk (odds ratio [OR] = 0.51, 95% confidence
interval [CI] = 0.34 to 0.76; P(trend)<.001) of prostate cancer
than those in the lowest category (<2.2 g/day).”
|
234
|
|
|
|
May
reduce the risk of getting a cold
|
“One
hundred forty-six volunteers were randomized to receive a placebo
or an allicin-containing garlic supplement, one capsule daily,
over a 12-week period between November and February… The
active-treatment group had significantly fewer colds than the
placebo group (24 vs 65, P < .001). The placebo group, in
contrast, recorded significantly more days challenged virally (366
vs 111, P < .05) and a significantly longer duration of
symptoms (5.01 vs 1.52 days, P < .001).”
|
235
|
|
|
Hot
peppers (capsaicin)
|
Associated
with higher rates of stomach cancer – in Mexicans who eat a LOT
|
“The
risk of [gastric cancer] was increased (OR = 1.71; 95% CI =
0.76-3.88) among high-level consumers of CAP (90-250 mg of
capsaicin per day, approximately 9-25 jalapeno peppers per day) as
compared to low-level consumers (0-29.9 mg of capsaicin per day,
approximately 0 to less than 3 jalapeno peppers per day; p for
trend p = 0.026)”
|
236
|
|
|
Lutein
and zeaxanthin
|
Associated
with lower risk of macula degeneration
|
A
review states that “Until scientifically sound knowledge is
available we recommend for patients judged to be at risk for AMD
to: alter their diet to more dark green leafy vegetables, wear UV
protective lenses and a hat when outdoors.”
|
237
|
|
|
|
Study
data showing a benefit is weak
|
“The
FDA recently reviewed intervention and observational studies that
evaluated the role of lutein and zeaxanthin in reducing the risk
of age-related macular degeneration and cataracts. On the basis of
this evidence-based review, the FDA concluded that no credible
evidence exists for a health claim about the intake of lutein or
zeaxanthin (or both) and the risk of age-related macular
degeneration or cataracts.”
|
238
|
|
|
|
Associated
with MUCH lower risk of prostate cancer (98% less in one
comparison)
|
These
are INCREDIBLE results. The odds ratios are truly extraordinary
(maybe unbelievably so), so I am including the entire abstract:
“To
determine whether dietary intake of lycopene and other carotenoids
has an etiological association with prostate cancer, a
case-control study was conducted in Hangzhou, southeast China
during 2001-2002. The cases were 130 incident patients with
histologically confirmed adenocarcinoma of the prostate. The
controls were 274 hospital inpatients without prostate cancer or
any other malignant diseases. Information on usual food
consumption, including vegetables and fruits, was collected by
face-to-face interviews using a structured food frequency
questionnaire. The risks of prostate cancer for the intake of
carotenoids and selected vegetables and fruits rich in carotenoids
were assessed using multivariate logistic regression, adjusting
for age, locality, education, income, body mass index, marital
status, number of children, family history of prostate cancer, tea
drinking, total fat and caloric intake. The prostate cancer risk
declined with increasing consumption of lycopene, alpha-carotene,
beta-carotene, beta-cryptoxanthin, lutein and zeaxanthin. Intake
of tomatoes, pumpkin, spinach, watermelon and citrus fruits
were also inversely associated with the prostate cancer risk. The
adjusted odds ratios for the highest versus the lowest quartiles
of intake were 0.18 (95% CI: 0.08-0.41) for lycopene,
0.43 (95% CI: 0.21-0.85) for alpha-carotene [from carrots,
squash, tomatoes etc.], 0.34 (95% CI: 0.17-0.69) for
beta-carotene, 0.15 (95% CI: 0.06-0.34) for
beta-cryptoxanthin [from red bell peppers, papaya,
cilantro, oranges etc.] and 0.02 (95% CI: 0.01-0.10) for
lutein and zeaxanthin. The corresponding dose-response
relationships were also significant, suggesting that vegetables
and fruits rich in lycopene and other carotenoids may be
protective against prostate cancer.”
|
239
|
|
|
|
Oil
is needed for good absorption
|
Lipids
from avocado (in salad) increased carotenoid absorption from salsa
by 2.6 to 4.4 times.
|
240
|
|
|
Fiber
|
Fruit
fiber and cereal fiber reduce heart risk
|
“We
analyzed the original data from 10 prospective cohort studies from
the United States and Europe to estimate the association between
dietary fiber intake and the risk of coronary heart disease….
After adjustment for demographics, body mass index, and lifestyle
factors, each 10-g/d increment of energy-adjusted and
measurement error–corrected total dietary fiber was associated
with a 14% … decrease in risk of all coronary events and a 27% …
decrease in risk of coronary death. For cereal, fruit, and
vegetable fiber intake [Relative Risks] corresponding to 10-g/d
increments were 0.90…, 0.84…, and 1.00 …, respectively, for
all coronary events and 0.75 …, 0.70 …, and 1.00…,
respectively, for deaths… Consumption of dietary fiber from
cereals and fruits is inversely associated with risk of coronary
heart disease.” Note: Vegetable fiber was NOT protective!
|
241
|
|
|
Citrus
rinds
|
Reduce
cholesterol
|
“Using
hamster models with diet-induced high cholesterol, the researchers
showed that feeding them food containing 1 percent [citrus
peel-derived] PMFs [(polymethoxylated flavones )] lowered levels
of LDL cholesterol by 32 to 40 percent.”
|
242
243
|
|
|
|
Reduce
the risk of cancer, both in people and rodents
|
“…case-control
study was designed to determine the usual citrus consumption
patterns of an older Southwestern population and to then evaluate
how this citrus consumption varied with history of squamous cell
carcinoma (SCC) of the skin… the most striking feature was the
protection purported by citrus peel consumption (OR = 0.66, 95% CI
= 0.45-0.95). Moreover, there was a dose-response relationship
between higher citrus peel in the diet and degree of risk
lowering.”
“Monoterpenes
are nonnutritive dietary components found in the essential oils of
citrus fruits and other plants. A number of these dietary
monoterpenes have antitumor activity. For example, d-limonene,
which comprises >90% of orange peel oil, has chemopreventive
activity against rodent mammary, skin, liver, lung and forestomach
cancers.”
How
in the world do you eat it? Remember marmalade, kumquats, and
fruitcake! Cooked citrus peel with added sweetener (I like
sucralose, but anything will do) adds spice to a berry mix. My
favorite combination is a mix of (mostly frozen berries)
blueberries, blackberries, raspberries, strawberries, cooked
orange peel and fiber mix (guar & psyllium [Wal-Mart’s
sugar-free Metamucil substitute]) spiced with sucralose &
ground cloves, moistened with red wine.
|
244
245
|
|
|
Vegan
diet
|
Not
more healthy than a lean meat + veggies diet
Better
for heart disease than the standard (“unhealthy”) diet.
|
“Just
cutting animal products out of your diet will not make you
healthier. … vegans tend to have worse mortality rates than
other groups.
The
largest meta-study to look at the relative merits of various diets
(in terms of rates of mortality) found: “There were no
significant differences between vegetarians and nonvegetarians in
mortality from cerebrovascular disease, stomach cancer, colorectal
cancer, lung cancer, breast cancer, prostate cancer, or all other
causes combined.”
However,
“Mortality from ischemic heart disease was 24% lower in
vegetarians than in nonvegetarians.”
|
246
247
|
|
|
Overview
|
A
summary of ways to prevent cancer, from JAMA
|
“Obesity
and overweight have been linked to development of several cancers,
including breast, colon, and uterine. Eating healthful foods in
smaller portions can help to reduce or maintain weight in a
healthful range.
• Eat
at least 5 servings of fruit and vegetables every day.
• Limit
your intake of saturated fats from meats, full-fat dairy products,
and processed foods.
• Include
high--fiber choices (whole-grain breads and cereals, raw fruits
and vegetables).
• Avoid
foods that have been charred or blackened because they may have
higher levels of carcinogens.....”
|
248
|
|
|
Vegetarian
diet needs supplements
|
B12
Taurine
|
|
|
|
|
Vegetarian
diet
|
Reduces
risk of heart disease
|
“A
cohort study of vegetarians and health-conscious persons in
Germany was followed-up prospectively for 21 years, including
1,225 vegetarians and 679 health-conscious nonvegetarians.
Standardized mortality ratios compared with the German general
population were calculated for all causes and specific
causes…RESULTS: Standardized mortality ratios for all-cause
mortality was significantly below 100: 59 [95% confidence interval
(95% CI), 54-64], predominantly due to a deficit of deaths from
circulatory diseases. Within the cohort, vegetarian compared with
nonvegetarian diet had no effect on overall mortality [rate ratio
(RR), 1.10; 95% CI, 0.89-1.36], whereas moderate and high physical
activity significantly reduced risk of death (RR, 0.62, 0.64),
adjusted for age, sex, smoking, alcohol intake, body mass index,
and educational level. Vegetarian diet was however associated
with a reduced RR of 0.70 (95% CI, 0.41-1.18) for ischemic heart
disease, which could partly be related to avoidance of meat.”
|
249
|
|
|
Fruit
|
Macula
degeneration
|
“We
conducted a prospective follow-up study of women in the Nurses'
Health Study and men in the Health Professionals Follow-up Study.
We followed 77 562 women and 40 866 men who were at least 50 years
of age and had no diagnosis of ARM or cancer at baseline for up to
18 years for women and up to 12 years for men. Fruit and vegetable
intakes were assessed with a validated semiquantitative
food-frequency questionnaire up to 5 times for women and up to 3
times for men during follow-up. RESULTS: A total of 464 (329 women
and 135 men) incident cases of early ARM and 316 (217 women and
99men) cases of neovascular ARM, all with visual loss of 20/30 or
worse due primarily to ARM, were diagnosed during follow-up. Fruit
intake was inversely associated with the risk of neovascular ARM.
Participants who consumed 3 or more servings per day of fruits had
a pooled multivariate relative risk of 0.64 (95% confidence
interval, 0.44-0.93; P value for trend =.004) compared with those
who consumed less than 1.5 servings per day. The results were
similar in women and men. However, intakes of vegetables,
antioxidant vitamins, or carotenoids were not strongly related to
either early or neovascular ARM. CONCLUSION: These data suggest a
protective role for fruit intake on the risk of neovascular ARM.”
|
250
|
|
|
|
Alzheimer
disease
|
“After
adjustment for potential confounders, the hazard ratio for
probable Alzheimer's disease was 0.24 (95% confidence interval
[CI], 0.09-0.61) comparing subjects who drank juices at least 3
times per week with those who drank less often than once per week
with a hazard ratio of 0.84 (95% CI, 0.31-2.29) for those
drinking juices 1 to 2 times per week (P for trend < .01). This
inverse association tended to be more pronounced among those with
an apolipoprotein Eepsilon-4 allele and those who were not
physically active.”
|
251
|
|
|
Blueberries
|
Brain
function
|
“…rats
given dietary supplements of fruit and vegetable extracts with
high antioxidant activity for 8 months beginning at 6 months of
age retarded age-related declines in neuronal and cognitive
function. The present study showed that such supplements
(strawberry, spinach, or blueberry …) fed for 8 weeks to
19-month-old Fischer 344 rats were also effective in reversing
age-related deficits in several neuronal and behavioral
parameters”
|
252
|
|
|
|
Mental
function in people
|
A
prospective, randomized study of 100 Americans age >60 showed
that “Among those receiving wild blueberries, significant
improvement occurred in decision speed (t-test p = 0.025) and
self-reported aches and pains (p = 0.017), energy level (p =
0.002), sharpness (p = 0.001), sleep quality (p = 0.017), mood (p
= 0.010), peacefulness (p = 0.005) and overall health (p = 0.001).
Blueberry group response times improved by 4.2%, decreasing from
39.96 to 38.27 centiseconds, more than twice the improvement in
the control group. Actual decision speeds were not displayed
during the study so speed improvement could not influence
self-reported health. Adjustments to balance decision speed
predictions, error rates and within-measurement decision-speed
improvement (our measures of expectation and motivation) in
blueberry and control groups did not significantly change these
results. Two blueberry recipients reported hearing improvement
that was confirmed by an independent observer”
|
253
|
|
|
Tomato
|
Lycopene
alone does not prevent prostate cancer; tomato does
|
“Consumption
of tomato powder but not lycopene inhibited prostate
carcinogenesis, suggesting that tomato products contain compounds
in addition to lycopene that modify prostate carcinogenesis.”
|
254
|
|
|
Pomegranate
|
|
From
a small study, pomegranate juice may help reduce carotid artery
stenosis.
|
255
|
|
|
|
|
A
moderate size prospective, randomized, double-blind study showed
decreased cardiac ischemia in heart disease patients who drank six
oz./day of pomegranate juice.
|
256
|
|
|
Red
grapefruit
|
Lowers
triglyceride levels
|
“Fifty-seven
hyperlipidemic patients, ages 39-72 years…During 30 consecutive
days of the investigation the diets of the patients of the red and
blond dietary groups were daily supplemented with one equal in
weight fresh red or blond grapefruit, respectively…Diet
supplemented with fresh red grapefruit positively influences serum
lipid levels of all fractions, especially serum triglycerides and
also serum antioxidant activity.”
|
257
|
|
|
Legumes
|
Associated
with long life in people
|
“The
'Food Habits in Later Life' (FHILL) is a cross-cultural study
conducted under the auspices of the International Union of
Nutritional Sciences (IUNS) and the World Health Organization
(WHO). Baseline data on food habits, health status and social
variables were collected from five cohorts aged 70 and over
(Japanese in Japan, Swedes in Sweden, Anglo-Celtic in Australia,
Greeks in Australia and Greece). Objective: To identify protective
dietary predictors amongst long-lived elderly people (n=785) …
Food items were grouped into nine food groups based on key
features of the Traditional Mediterranean Diet (vegetables,
legumes, fruits and nuts, cereals (including starchy roots), dairy
products, meat, fish, monounsaturated: saturated ratio, and
ethanol). All-cause mortality data were obtained from up to seven
years follow-up. Alternative Cox Proportional Hazard model
adjusted to age at enrolment (in 5-year interval), gender, and
smoking was developed to analyse the survival data...Results: Only
for legumes intake was the result plausible, consistent and
statistically significant across collective FHILL cohort's data.
There is a 7% - 8% reduction in mortality hazard ratio for
every 20g increase in daily legume intake with adjustment for
location/ethnicity …The significance of legumes persisted even
after controlling for age at enrolment (in 5-year interval),
gender, and smoking. Legumes have been associated with long-lived
food cultures such as the Japanese (soy, tofu, natto, miso), the
Swedes (brown beans, peas), and the Mediterranean people (lentils,
chickpeas, white beans).”
|
258
|
|
|
|
Associated
with reduced risk of prostate cancer
|
“multicenter
case-control study …Intake of legumes (whether total legumes,
soyfoods specifically, or other legumes) was inversely related to
prostate cancer (OR for highest relative to lowest quintile for
total legumes = 0.62; P for trend = 0.0002); …Intakes of
yellow-orange and cruciferous vegetables were also inversely
related to prostate cancer, especially for advanced cases, among
whom the highest quintile OR for yellow-orange vegetables = 0.67
(P for trend = 0.01) and the highest quintile OR for cruciferous
vegetables = 0.61 (P for trend = 0.006). Intake of tomatoes and of
fruits was not related to risk. Findings were generally consistent
across ethnic groups. These results suggest that legumes (not
limited to soy products) and certain categories of vegetables may
protect against prostate cancer.”
|
259
|
|
Go
to TOC
Alcohol
and wine
Wine
or purple grape juice – the jury is still out. Purple grape juice
in moderate amounts is probably good for you; if you are a man over
40 or a woman over 50 you could substitute a small glass of
red wine (Circulation
2001 Jan 23;103(3):472-5; PMID: 11157703)
each day. There is some evidence that alcohol itself has an
independent beneficial effect in small quantities by increasing HDL
levels, or possibly by the anti-AGE effect of its metabolite
acetaldehyde (Proc
Natl Acad Sci U S A 1999 Mar 2;96(5):2385-90; PMID: 10051651).
. In addition, for men who drink moderately at least 5 days per week
there is also a 36% reduction in the incidence of diabetes (Diabetes
2001 Oct;50(10):2390-5; PMID: 11574424).
A drink of any kind of alcohol beverage 3 to 5 times per week seems
to reduce the risk of heart attack in men by about 35% in a large
recent study (Mukamal
KJ, Conigrave KM, Mittleman MA, Camargo CA Jr, Stampfer MJ, Willett
WC, Rimm EB. Roles of drinking pattern and type of alcohol consumed
in coronary heart disease in men. N Engl J Med. 2003 Jan
9;348(2):109-18. PMID: 12519921.)
Polyphenols may be the active component, and these may be more potent
in red wine than in grape juice. Red wine has the same antioxidants
found in purple grape juice. Apparently white wine or other drinks
with alcohol may not be helpful. Burgundy and cabernet sauvignon
(perhaps these are the same thing?) have the highest antioxidant
level of those tested in vitro.
Light alcohol intake
also seems to be associated with a smaller risk of strokes (Stroke
2001 Sep;32(9):1939-46; PMID: 11546878);
however the same study showed that there is dose-dependant shrinkage
of the brain with alcohol use, and long-term,
moderate or high intake of alcohol is one of the causes of cancer
(but on the other hand, the catechins in red wine help to prevent
cancer in animals American
Journal of Clinical Nutrition, Vol. 76, No. 4, 865-872, October 2002)
In other words, you might have a smaller risk of strokes per se but
gradually lose your brain in the process from the toxic effects of
alcohol. Another recent study of 6500 patients in Britain showed a
lower rate of cardiovascular disease among those who drank
moderately, but the overall death rate from all causes was actually
larger. Wine may be associated with lower risk of dementia (Truelsen
T, Thudium D, Gronbaek M; Copenhagen City Heart Study. Amount and
type of alcohol and risk of dementia: the Copenhagen City Heart
Study. Neurology. 2002 Nov 12;59(9):1313-9. PMID: 12427876),
but it is possible that associated factors other than wine may be at
work (e.g. perhaps those who drink wine have a better lifestyle), or
factors in the wine other than alcohol. To my gestalt, it is better
if you can control your risk for stroke and heart attack by other
means than alcohol (diet, aspirin, blood pressure control).
Problems: Alcohol has several risks: alcoholism, especially
if you are young or genetically prone to it, breast cancer (“results
suggest that about 4% of the breast cancers in developed countries
are attributable to alcohol.” Alcohol,
tobacco and breast cancer - collaborative reanalysis of individual
data from 53 epidemiological studies, including 58 515 women with
breast cancer and 95 067 women without the disease. Br J Cancer. 2002
Nov 18;87(11):1234-1245. PMID: 12439712),
other cancers, hypertension, and stroke. The metabolite of ethanol
(acetaldehyde) is itself toxic, with hundreds of articles about its
toxicity. And worst of all, about 10% of all people may be
susceptible to alcoholism: this is most likely in those who start
drinking at a young age. These are the reasons for the age
recommendations. For many people (and indeed in general!) it may not
be worth drinking any wine at all.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Alcohol
|
Reduces
dementia and cognitive loss
|
Moderate
drinking among the elderly is associated with half the risk of
dementia. “Compared with abstention, consumption of 1 to 6
drinks weekly is associated with a lower risk of incident dementia
among older adults.”
Michael
Rae (CR society list, 2004-10-14) did a careful review of eleven
studies on the effects of alcohol on dementia, and concluded that
“The evidence on alcohol & dementia shows a clear trend
toward a protective effect, most clearly for wine”
|
260
261
|
|
|
|
|
From
the Nurses Health Study “Our data suggest that in women, up to
one drink per day does not impair cognitive function and may
actually decrease the risk of cognitive decline.”
|
262
|
|
|
|
Reduced
risk of ischemic stroke
|
“After
adjusting for other risk factors compared with those who did not
drink in the past year, moderate drinkers had a reduced risk of IS
(0.67; 95% CI, 0.46 to 0.99) and IS, myocardial infarction, or
vascular death (0.74; 95% CI, 0.59 to 0.94).”
|
263
|
|
|
|
Reduces
risk of CVD (heart disease)
|
“From
the Physicians' Health Study enrollment cohort of 88 882 men who
provided self-reported information on alcohol intake, we
identified a group of 14 125 men with a history of current or past
treatment for hypertension who were free of myocardial infarction,
stroke, cancer, or liver disease at baseline…These results,
which require confirmation in other large-scale studies, suggest
that light to moderate alcohol consumption is associated with a
reduction in risk of total and CVD mortality in hypertensive men.”
|
264
|
|
|
|
|
“This
cross-sectional study was performed using data from the
population-based Rotterdam Coronary Calcification Study. Data on
alcohol consumption were available for 1795 individuals without
coronary heart disease. Mean +/- SD age of the participants was 71
+/- 5.7 years. Coronary calcification was detected on electron
beam computed tomographic scans and quantified as a calcium score
by the Agatston method… A U-shaped association was found between
alcohol consumption and coronary calcification…The risk of
extensive coronary calcification was 50% lower in individuals who
consumed 1 to 2 alcoholic drinks per day than in nondrinkers.”
|
265
|
|
|
|
Reduces
all-cause mortality
|
This
epidemiologic study for 10 years found that moderate alcohol
reduces all-cause mortality in men after age 35. However,
before age 35, it increases the risk of death. Makes sense to me:
young men may die of accidents and violence due to alcohol.
|
266
|
|
|
|
|
“We
undertook a 23-year prospective study of 12 000 male British
doctors aged 48-78 years in 1978…ischaemic heart disease (RR
0.72, CI 0.58-0.88, P = 0.002), respiratory disease (RR 0.69, CI
0.52-0.92, P = 0.01), and all-cause (RR 0.88, CI 0.79-0.98, P =
0.02) mortality were significantly lower than in the
non-drinkers.”
|
267
|
|
|
|
|
“We
performed a meta-analysis of prospective studies on alcohol
dosing and total mortality. METHODS: We searched PubMed for
articles available until December 2005, supplemented by references
from the selected articles. Thirty-four studies on men and women,
for a total of 1 015 835 subjects and 94 533 deaths, were
selected. Data were pooled with a weighed regression analysis of
fractional polynomials. RESULTS: A J-shaped relationship between
alcohol and total mortality was confirmed in adjusted studies, in
both men and women. Consumption of alcohol, up to 4 drinks per
day in men and 2 drinks per day in women, was inversely associated
with total mortality, maximum protection being 18% in women (99%
confidence interval, 13%-22%) and 17% in men (99% confidence
interval, 15%-19%). Higher doses of alcohol were associated with
increased mortality... CONCLUSIONS: Low levels of alcohol
intake (1-2 drinks per day for women and 2-4 drinks per day for
men) are inversely associated with total mortality in both men and
women.”
|
268
|
|
|
|
Increases
breast cancer risk (by a small amount)
|
“Compared
with women who reported drinking no alcohol, the relative risk of
breast cancer was 1.32 (1.19-1.45, P<0.00001) for an intake of
35-44 g per day alcohol, and 1.46 (1.33-1.61, P<0.00001) for
>/=45 g per day alcohol. The relative risk of breast cancer
increased by 7.1% (95% CI 5.5-8.7%; P<0.00001) for each
additional 10 g per day intake of alcohol, i.e. for each extra
unit or drink of alcohol consumed on a daily basis… If the
observed relationship for alcohol is causal, these results suggest
that about 4% of the breast cancers in developed countries are
attributable to alcohol.”
|
269
|
|
|
|
Increases
the risk of hypertension
|
“drinking
outside meals appears to have a significant effect on hypertension
risk independent of the amount of alcohol consumed.”
|
270
|
|
|
|
|
For
40 gm alcohol per day, “compared with control-abstinence, both
red wine and beer increased awake systolic BP (2.9 and 1.9 mm
Hg, respectively; P<0.05) and asleep [heart rate] (5.0 and 4.4
bpm; P<0.05).”
|
271
|
|
|
|
… but
moderate amounts are safe
|
“Heavy
alcohol consumption increases risk for hypertension, which is in
itself a strong risk factor for cardiovascular disease (CVD)...
OBJECTIVE: To assess whether alcohol consumption is inversely
associated with CVD among men with hypertension. DESIGN:
Prospective cohort study. SETTING: United States.
PARTICIPANTS: 11,711 men with hypertension from the Health
Professionals Follow-Up Study. MEASUREMENTS: Alcohol consumption
was assessed every 4 years by using a food-frequency
questionnaire. Incident cases of nonfatal myocardial infarction
(MI), fatal coronary heart disease, and stroke were documented
from 1986 to 2002. RESULTS: During follow-up, 653 patients with MI
were documented. Compared with patients abstaining from
alcohol, the hazard ratio for participants with MI consuming 0.1
to 4.9 grams of alcohol per day was 1.09 (95% CI, 0.86 to 1.37);
consuming 5 to 9.9 grams of alcohol per day was 0.81 (CI, 0.60 to
1.08 g/d); consuming 10 to 14.9 grams of alcohol per day was 0.68
(CI, 0.51 to 0.91 g/d); consuming 15 to 29.9 grams of alcohol per
day was 0.72 (CI, 0.54 to 0.97 g/d); consuming 30 to 49.9 grams of
alcohol per day was 0.67 (CI, 0.48 to 0.94 g/d); and consuming 50
or more grams of alcohol per day was 0.41 (CI, 0.22 to 0.77 g/d)
(P < 0.001 for trend). Associations were similar for fatal
and nonfatal MI. Alcohol consumption was not associated with total
death or death due to CVD. Risks for total and ischemic stroke
for patients consuming 10 to 29.9 g of alcohol per day were 1.40
(CI, 0.93 to 2.12) and 1.55 (CI, 0.90 to 2.68) compared with that
of abstainers... CONCLUSIONS: In this population of men with
hypertension, moderate alcohol consumption was associated with a
decreased risk for MI but not with risks for total death or death
due to CVD.”
|
272
|
|
|
Red
wine
|
May
decrease risk of prostate cancer
|
“Each
additional glass of red wine consumed per week showed a
statistically significant 6% decrease in relative risk”
|
273
|
|
|
|
Resveratrol
(found in red wine) improves lifespan in mice
|
“resveratrol
shifts the physiology of middle-aged mice on a high-calorie diet
towards that of mice on a standard diet and significantly
increases their survival.”
|
274
|
|
Go
to TOC
Fiber
Personal
note: I find glucomannan the most palatable and easy to use fiber. I
like to mix it with my food, often with spices (garlic, onion powder
& NuSalt). All soluble fibers absorb more fluid over time, so go
easy at first. You may find your stomach swelling up as the day goes
on. It is most effective at slowing absorption of glucose when mixed
with food.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Soluble
fiber
|
Glucomannan
|
A
randomized clinical trial showed that daily glucomannan
“supplement improved blood lipid levels by enhancing fecal
excretion of neutral sterol and bile acid and alleviated the
elevated glucose levels in diabetic subjects.” It reduced
cholesterol by 11% and LDL by 20%.
|
275
|
|
|
|
|
“Decreases
in serum cholesterol (total, 12.4+/-3.1%, P<0.004; LDL,
22+/-3.9%, P<0.002; total/HDL ratio, 15.2+/-3.4%, P<0.003;
and LDL/HDL ratio, 22.2+/-4.1%, P< 0.002), apolipoprotein (apo)
B (15.1+/-4.3%, P<0.0004), apo B/A-1 ratio (13.1+/-3.4%, P<
0.0003), and serum fructosamine (5.2+/-1.4%, P<0.002) were
observed during [glucomannan] treatment compared with [wheat
bran]-control. Fasting blood glucose, insulin, triglycerides, HDL
cholesterol, and body weight remained unchanged. CONCLUSIONS: A
diet rich in high-viscosity KJM improves glycemic control and
lipid profile, suggesting a therapeutic potential in the treatment
of the insulin resistance syndrome.”
|
276
|
|
|
|
Notes
on soluble fiber, such as which soluble fiber type best?
|
Glucomannan
is white, is very easy to mix, has no taste and absorbs a huge
amount of water. It is very useful in preparing foods – use it
like corn starch. Downside: expense.
Guar
is hard to mix (unless mixed in with something else like
psyllium), and has a distinct taste. Needs to be very finely
ground up.
Psyllium:
Good against constipation. Needs to be ground finely (don’t get
the rough stuff).
|
|
|
|
|
Psyllium
reduces hunger and postprandial glucose levels
|
In
a randomized, controlled clinical trial: “After the meal, hunger
feelings and energy intake were significantly lower during the
psyllium session than during the placebo session (13% and 17%
lower respectively; P < 0.05). Postprandial increase in serum
glucose, triglycerides and insulin levels was less with psyllium
than with placebo (P < 0.05).”
|
277
|
|
|
|
Protects
against carotid blood vessel narrowing
Raises
HDL
|
“A
significant inverse association was observed between IMT
progression and the intakes of viscous fiber (P = 0.05)
and pectin (P = 0.01). Correction for measurement
error increased the magnitude of these estimated
effects. The ratio of total to HDL cholesterol was
inversely related to the intakes of total fiber (P
= 0.01), viscous fiber (P = 0.05), and pectin (P =
0.01).”
|
278
|
|
|
|
Reduces
the rise in blood glucose with a meal
|
“guar
gum supplementation attenuated the blood glucose response after
the meals”
|
279
|
|
|
|
|
“Varying
the amount of psyllium incorporated into the cereal from 0 to 20%
resulted in a linear dose-dependent reduction of the glycemic
index (GI) (GI = 101 -2.2 x % psyllium; r = 0.950; p less than
0.002)…the mechanism of action relates to a reduced rate of
digestion rather than carbohydrate malabsorption.”
|
280
|
|
|
|
|
“A
high intake of dietary fiber, particularly of the soluble type,
above the level recommended by the ADA, improves glycemic control,
decreases hyperinsulinemia, and lowers plasma lipid concentrations
in patients with type 2 diabetes.”
|
281
|
|
|
|
Reduces
blood pressure
|
“Results
suggest that a diet containing soluble fiber-rich whole oats can
significantly reduce the need for antihypertensive medication and
improve BP control. Considering the lipid and glucose improvements
as well, increased consumption of whole oats may significantly
reduce cardiovascular disease risk.”
|
282
|
|
|
Fiber
|
Reduces
LDL
Reduces
colon cancer risk factors
|
“The
diets were: high-vegetable, fruit, and nut (very-high-fiber, 55
g/1,000 kcal)… Compared with the starch-based and low-fat diets,
the high-fiber vegetable diet resulted in the largest reduction in
low-density lipoprotein (LDL) cholesterol (33% +/- 4%, P <.001)
and the greatest fecal bile acid output (1.13 +/- 0.30 g/d, P
=.002), fecal bulk (906 +/- 130 g/d, P <.001), and fecal
short-chain fatty acid outputs (78 +/- 13 mmol/d, P <.001).
Nevertheless, due to the increase in fecal bulk, the actual
concentrations of fecal bile acids were lowest on the vegetable
diet (1.2 mg/g wet weight, P =.002). Maximum lipid reductions
occurred within 1 week… We conclude that very high-vegetable
fiber intakes reduce risk factors for cardiovascular disease and
possibly colon cancer.”
|
283
|
|
|
|
Reduces
CRP levels (likely to => reduced risk of heart disease)
|
“We
examined the association between dietary fiber and
serum concentration of C-reactive protein (CRP), a
possible predictor of cardiovascular events, using data
from the National Health and Nutrition Examination Survey
1999–2000. Among 3920 participants
20
y old, dietary fiber intake was inversely associated
with serum CRP concentration. The [adjusted] odds ratio
(OR) for increased CRP concentration (>3.0 mg/L) was
… 0.59…Our findings indicate that fiber intake is
independently associated with serum CRP concentration
and support the recommendation of a diet with a high
fiber content.”
|
284
|
|
Go
to TOC
Hypertension
and salt (see also CR, Exercise)
Keep
your blood pressure lower than 129/85 (both numbers are
important, and optimal BP is < 115/75), no matter your age. The
longest study (25 years follow-up on 10,874 patients) showed that
Life expectancy was shortened by 2.2 years for men with high-normal
blood pressure and by 4.1 years for those with stage 1 hypertension,
where high-normal is a reading of 130-139 (systolic pressure) over
85-89 (diastolic pressure) and stage 1 hypertension is 140-159 over
90-99.
A huge review of blood pressure studies on 1 million
patients showed that there is a two-fold increase in risk of death
from stroke or ischemic heart disease, no matter the baseline blood
pressure (down to at least 115/75) and no matter the age (within the
age range of 40-89 yr). “Throughout middle and old age,
usual blood pressure is strongly and directly related to vascular
(and overall) mortality, without any evidence of a threshold down to
at least 115/75 mm Hg.” (Prospective Studies
Collaboration. Age-specific relevance of usual blood pressure to
vascular mortality: a meta-analysis of individual data for one
million adults in 61 prospective studies. Lancet 2002; 360:
1903-13.)
A
DASH diet (low salt, low fat, high vegetables and fruit diet) can
lower your blood pressure by 7 to 11 mm Hg,
and again Miller
ER 3rd, Erlinger TP, Young DR, Jehn M, Charleston J, Rhodes D, Wasan
SK, Appel LJ. Results of the Diet, Exercise, and Weight Loss
Intervention Trial (DEW-IT). Hypertension. 2002 Nov;40(5):612-8.
PMID: 12411452. Note that caloric
restriction does this by its
nature: by reducing the amount of calories there is usually a
natural reduction in the amount of saturated fat and salt intake –
another good reason to practice caloric restriction, if you need one.
In practice, those who practice caloric restriction typically seem to
drop their blood pressure by 10-20 mm Hg! Two other methods that seem
to have merit in reducing BP are moderate exercise and reducing
alcohol intake.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Blood
pressure
|
Lower
is MUCH better
|
“At ages 40-69
years, each difference of 20 mm Hg usual SBP (or, approximately
equivalently, 10 mm Hg usual DBP) is associated with more than a
twofold difference in the stroke death rate, and with twofold
differences in the death rates from IHD and from other vascular
causes. …Throughout middle and old age, usual blood pressure is
strongly and directly related to vascular (and overall) mortality,
without any evidence of a threshold down to at least 115/75 mm
Hg.” Note: SBP = Systolic Blood Pressure; DBP = Diastolic Blood
Pressure.
|
285
|
|
|
|
|
A
population based “prospective study of a random sample of 1700
Danish men and women, aged 41 to 72 years” found both
cardiovascular death and all-cause mortality over a period
averaging 9.5 years. The cardiovascular death relative risk for
“10 mm Hg increments in systolic and 5 mm Hg increments in
diastolic ambulatory blood pressure were 1.51 (1.28 to 1.77) and
1.43 (1.26 to 1.61). The corresponding figures for all cause
mortality were 1.18 (1.06 to 1.31) and 1.18 (1.09 to 1.28)”
|
286
|
|
|
|
|
Richard
Martin, a senior lecturer in epidemiology and public health at the
University of Bristol in Britain stated “A one percent
reduction in population systolic blood pressure levels is
associated with about a 1.5 percent reduction in all-cause
mortality”
|
287
|
|
|
|
Higher
BP reduces brain function at all ages
|
“In this
20-year longitudinal study, we examined the relationship between
baseline blood pressure and cognitive decline for 529 participants
using 2 age groups (18 to 46 years and 47 to 83 years)… Results
indicated that higher levels of baseline systolic blood pressure,
diastolic blood pressure, mean arterial pressure, and blood
pressure categories … were significantly associated with decline
in Visualization/Fluid abilities in both younger and older age
groups. Young adults are as susceptible to blood pressure-related
longitudinal decline in cognitive performance as are older
adults.”
“Cerebral white
matter lesions are frequently observed on magnetic resonance
imaging (MRI) scans in elderly people and are associated with
stroke and dementia… 1805 nondemented subjects aged 65 to 75
years were sampled from ongoing community-based studies that were
initiated 5 to 20 years before the MRI. …We performed logistic
regression analyses adjusted for potential confounders in 1625
people with complete data. Concurrently and formerly assessed
diastolic and systolic blood pressure levels were positively
associated with severe white matter lesions… Higher blood
pressure was associated with an increased risk of severe white
matter lesions.”
“Controlling
for potential confounders, each 10 mmHg increase in supine SBP
was associated with a 2.31-fold increase … in risk for
impairment in psychomotor speed and set shifting”
“For
each additional year of [hypertension] treatment there was a
reduction in the risk of incident dementia (hazard ratio
[HR]=0.94, 95% CI, 0.89 to 0.99)... Results suggest that in
hypertensive men, the duration of the antihypertensive treatment
is associated with a reduced risk for dementia and cognitive
decline.”
|
288
289
290
291
|
|
|
Salt
reduction, exercise, weight loss, reducing alcohol
|
Lower
hypertension
|
A
US Government NIH summary of “Prevention of Primary
Hypertension” is available as a PDF file. A summary of the
most-proven approaches to prevention of hypertension is on page
17, and recommends:
1. Exercise 30 minutes/day
2.
Maintain a low BMI (18.5-24.9)
3. Limit alcohol
to essentially no more than one drink/day
4. Reduce salt
intake to < 6 gm/day
5. Get enough dietary potassium
6.
Good diet: fruits, vegetables, low-fat dairy, low in saturated
and total fat (the DASH diet)
|
292
|
|
|
Exercise
|
|
“Vigorous
exercise reduces day time ambulatory BP and, in combination with
calorie restriction, had a synergist effect to reduce night-time
and 24 h BP. 4. Exercise is a positive and effective adjunct to
other lifestyle measures in the prevention of hypertension.
Adherence to either supervised or unsupervised moderate-intensity
exercise is sufficient to reduce BP in the short and long term.”
|
293
|
|
|
Salt
|
There
is a linear effect of salt intake on BP => stroke and heart
attack
|
“A
reduction of 3 g/d predicts a fall in blood pressure of
3.6 to 5.6/1.9 to 3.2 mm Hg (systolic/diastolic) in hypertensives
and 1.8 to 3.5/0.8 to 1.8 mm Hg in normotensives. The effect
would be doubled with a 6 g/d reduction and tripled with a 9
g/d reduction. A conservative estimate indicates that a
reduction of 3 g/d would reduce strokes by 13% and
ischemic heart disease (IHD) by 10%.”
|
294
|
|
|
|
The
Institute of Medicine recommends 1.5 gm sodium/day and >
4.7 gm potassium/day
|
“The
Institute of Medicine serves as adviser to the nation to improve
health. As an independent, scientific adviser, the Institute of
Medicine strives to provide advice that is unbiased, based on
evidence, and grounded in science.” On 2004-02-11 they
recommended 1.5 gm sodium/day (down from 2.4 gm), and to get far
more dietary potassium than is now common.
|
295
|
|
|
|
High
salt intake is associated with high risk for gastric cancer
|
“…
the frequency
categories of highly salted foods such as salted fish roe and
salted fish preserves were strongly associated with the risk in
both sexes. Restriction of salt and salted food intake is a
practical strategy to prevent gastric cancer in areas with high
risk.”
|
296
|
|
|
|
Salt
reduction reduces blood pressure in children too
|
“To
assess the effect of reducing salt intake on blood pressure in
children, we carried out a meta-analysis of controlled
trials…Ten trials of children and adolescents with 966
participants …Salt intake was reduced by 42% (interquartile
range [IQR]: 7% to 58%). There were significant reductions in
blood pressure: systolic: -1.17 mm Hg (95% CI: -1.78 to -0.56 mm
Hg; P<0.001); diastolic: -1.29 mm Hg (95% CI: -1.94 to -0.65 mm
Hg; P<0.0001)… a modest reduction in salt intake causes
immediate falls in blood pressure and, if continued, may well
lessen the subsequent rise in blood pressure with age. This would
result in major reductions in cardiovascular disease. These
results in conjunction with other evidence provide strong support
for a reduction in salt intake in children.”
|
297
|
|
|
Potassium
|
Lowers
BP
|
A
review of randomized trials found: “A total of 40 sodium trials
and 27 potassium trials in adults with a minimum duration of 2
weeks were selected for analysis… Sodium reduction (median: -77
mmol/24 h) was associated with a change of -2.54 mmHg (95% CI:
-3.16, -1.92) in systolic blood pressure and -1.96 mmHg (-2.41,
-1.51) in diastolic blood pressure. Corresponding values for
increased potassium intake (median: 44 mmol/24 h) were -2.42 mmHg
(-3.75, -1.08) and -1.57 mmHg (-2.65, -0.50). Blood pressure
response was larger in hypertensives than normotensives, both for
sodium (systolic: -5.24 vs -1.26 mmHg, P < 0.001; diastolic:
-3.69 vs -1.14 mmHg, P < 0.001) and potassium (systolic: -3.51
vs -0.97 mmHg, P=0.089; diastolic: -2.51 vs -0.34 mmHg, P=0.074).”
Bottom line: get more potassium and less sodium!
|
298
|
|
|
|
|
A
recent summary measures to prevent hypertension states that
“…modifiable factors might decrease blood pressure and even
prevent the development of hypertension. Thus, present national
recommendations and guidelines include lifestyle modifications
ranging from weight loss in case of obesity, engagement in
regular isotonic physical activity, reduced sodium
diet (<100 mmol/d), supplementation of potassium, and
alcohol moderation (<1 ounce of ethanol or its
equivalent per day).”
|
299
|
|
|
|
|
Adding
KCl or K citrate to the diet reduces blood pressure. This study of
hypertensives found a ~12 point systolic and 5 point diastolic BP
reduction.
|
300
|
|
|
|
Lowers
rate of cardiovascular disease deaths in the elderly
|
“Five
kitchens of a veteran retirement home were randomized into 2
groups (experimental or control) and veterans assigned to those
kitchens were given either potassium-enriched salt (experimental
group) or regular salt (control group) for approximately 31 mo.
Information on death, health insurance claims, and dates that
veterans moved in or out of the home was gathered. RESULTS:
Altogether, 1981 veterans, 768 in the experimental [x (+/-SD) age:
74.8 +/- 7.1 y] and 1213 in the control (age: 74.9 +/- 6.7 y)
groups, were included in the analysis. The experimental group had
better CVD survivorship than did the control group. The incidence
of CVD-related deaths was 13.1 per 1000 persons (27 deaths in 2057
person-years) and 20.5 per 1000 (66 deaths in 3218 person-years)
for the experimental and control groups, respectively. A
significant reduction in CVD mortality (age-adjusted hazard ratio:
0.59; 95% CI: 0.37, 0.95) was observed in the experimental group.
Persons in the experimental group lived 0.3-0.90 y longer and
spent significantly less ( approximately US $426/y) in inpatient
care for CVD than did the control group, after control for age and
previous hospitalization expenditures…The effect was likely due
to a major increase in potassium and a moderate reduction in
sodium intakes.”
|
301
|
|
|
Vegetables
and fruit
|
Lower
BP
|
A
7-year study found that a “prospective cohort study of 1,710
employed men in Chicago, Illinois, initially aged 41-57 years…
diets higher in fruits and vegetables and lower in meats (except
fish) may reduce the risk of developing high BP.”
|
302
|
|
|
|
|
“In
a Mediterranean population with an elevated [vegetable] fat
consumption, a high fruit and vegetable intake is inversely
associated with BP levels.”
|
303
|
|
|
Vegetarian
diet
|
Lowers
BP
|
“Evidence
that vegetarian dietary patterns lower blood pressure (BP) comes
from both population studies and randomized controlled trials in
normotensive and hypertensive subjects. 2. The effect has been
shown most clearly in those who keep to a strict lacto-ovo
vegetarian diet characterized by a relatively low intake of
saturated fat, a high polyunsaturated/saturated fat ratio, and a
high intake of fruit, vegetables and other fibre containing
products. Randomized controlled dietary trials suggest the effects
are independent of dietary sodium, additive to that of calorie
restriction, and not due to the absence of meat protein per se.”
|
304
|
|
|
Melatonin
|
|
“We
conducted a randomized, double-blind, placebo-controlled,
crossover trial in 16 men with untreated essential hypertension to
investigate the influence of acute (single) and repeated (daily
for 3 weeks) oral melatonin (2.5 mg) intake 1 hour before sleep on
24-hour ambulatory blood pressure … Repeated melatonin intake
reduced systolic and diastolic blood pressure during sleep by 6
and 4 mm Hg, respectively. … Repeated (but not acute) melatonin
also improved sleep… In patients with essential hypertension,
repeated bedtime melatonin intake significantly reduced nocturnal
blood pressure.”
|
305
|
|
|
Protein
|
High
protein intake diet is correlated with a small decrease in BP
|
Note:
this type of study is fraught with potential problems. In an
Okinawan cohort, “…both [systolic] BP and [diastolic] BP
tended to be lower in those with higher daily protein intake,
particularly in men.”
|
306
|
|
|
|
|
A
randomized control trial showed that both high protein and soluble
vegetable fiber (from psyllium in this case) significantly lower
blood pressure. “Relative to control subjects, the net reduction
in 24-hour systolic blood pressure was 5.9 mm Hg with fiber and
with protein. Findings were independent of age, gender, and change
in weight, alcohol intake, or urinary sodium and potassium.
Relative to reduced fiber and protein intake, dietary protein
and soluble fiber supplements lower blood pressure additively in
hypertensives.”
|
307
|
|
|
Protein
and MUFAs
|
Reduce
BP and improve lipids
|
“Randomized,
3-period, crossover feeding study … Participants were 164 adults
with prehypertension or stage 1 hypertension. Each feeding period
lasted 6 weeks and body weight was kept constant. INTERVENTIONS: A
diet rich in carbohydrates; a diet rich in protein, about half
from plant sources; and a diet rich in unsaturated fat,
predominantly monounsaturated fat. MAIN OUTCOME MEASURES: Systolic
blood pressure and low-density lipoprotein cholesterol. RESULTS:
Blood pressure, low-density lipoprotein cholesterol, and estimated
coronary heart disease risk were lower on each diet compared with
baseline. Compared with the carbohydrate diet, the protein diet
further decreased mean systolic blood pressure by 1.4 mm Hg (P
= .002) and by 3.5 mm Hg (P = .006) among those with hypertension
and decreased low-density lipoprotein cholesterol by 3.3 mg/dL
(0.09 mmol/L; P = .01), high-density lipoprotein cholesterol by
1.3 mg/dL (0.03 mmol/L; P = .02), and triglycerides by 15.7 mg/dL
(0.18 mmol/L; P<.001). Compared with the carbohydrate diet, the
unsaturated fat diet decreased systolic blood pressure by 1.3
mm Hg (P = .005) and by 2.9 mm Hg among those with
hypertension (P = .02), had no significant effect on low-density
lipoprotein cholesterol, increased high-density lipoprotein
cholesterol by 1.1 mg/dL (0.03 mmol/L; P = .03), and lowered
triglycerides by 9.6 mg/dL (0.11 mmol/L; P = .02). Compared
with the carbohydrate diet, estimated 10-year coronary heart
disease risk was lower and similar on the protein and unsaturated
fat diets.”
|
308
|
|
|
Olive
oil
|
Associated
with lower BP
|
“Olive
oil intake…is inversely associated with both systolic
and diastolic blood pressure.”
|
309
|
|
|
|
|
“We
evaluated the effects of a moderate consumption of olive oil on
lipid profile, BMI, and blood pressure (BP) in a group of 160
healthy men …The study was a randomized, cross-over trial
…General linear models showed that the administration of the
sequence of the 3 olive oils was responsible for a 3% decrease in
systolic BP (SBP) (P < 0.05), but not in diastolic BP, in the
non-Mediterranean subjects… this study suggest that a moderate
consumption of olive oil may be used as an effective tool to
reduce SBP of healthy men who do not typically consume a
Mediterranean diet.”
|
310
|
|
|
Folate
at high doses (5 mg/day – 8 times more than the RDA)
|
Lowers
BP
|
“Forty-one
asymptomatic men with normal or high-normal ambulatory blood
pressure (systolic: >130 to <145 mm Hg; diastolic: >80 to
<90 mm Hg) participated. The study had a randomized,
placebo-controlled, double-blind, crossover design that
incorporated 3-wk treatments with 5 mg folic acid/d or matching
placebo; each treatment was separated by a 4-wk washout phase.
RESULTS: Folic acid reduced brachial pulse pressure by 4.7 +/- 1.6
mm Hg (P < 0.05) without changing mean arterial pressure…Folic
acid is a safe and effective supplement that targets large artery
stiffness and may prevent isolated systolic hypertension.”
|
311
|
|
|
Low
fat dairy
|
Associated
with lower rate of HTN (only low-fat dairy)
|
“a
prospective study conducted in 5880 university graduates in Spain,
aged >20 y in 2000 (x age: 37 y), free of hypertension and
cardiovascular disease at baseline, and followed-up with mailed
questionnaires for a median of 27 mo…One hundred eighty new
cases of hypertension were identified. The hazard ratio of
hypertension between extreme quintiles of low-fat dairy product
consumption was 0.46 (95% CI: 0.26, 0.84; P for trend = 0.02)
after adjustment for the main known risk factors for hypertension
and several dietary factors… low-fat dairy consumption, but not
whole-fat dairy consumption, was associated with a lower risk of
incident hypertension.”
|
312
|
|
|
|
|
“5880
university graduates in Spain … mean age: 37 y … followed-up
with mailed questionnaires for a median of 27 mo… One hundred
eighty new cases of hypertension were identified. The hazard ratio
of hypertension between extreme quintiles of low-fat dairy product
consumption was 0.46 (95% CI: 0.26, 0.84; P for trend = 0.02)
after adjustment for the main known risk factors for hypertension
and several dietary factors. No significant association between
whole-fat dairy products or total calcium intake and incident
hypertension was seen.”
|
313
|
|
|
Sleep
|
<
5 hr/night raises BP (obesity risk too)
|
“Sleep
durations of </=5 hours per night were associated with a
significantly increased risk of hypertension (hazard ratio, 2.10;
95% CI, 1.58 to 2.79) in subjects between the ages of 32 and 59
years, and controlling for the potential confounding variables
only partially attenuated this relationship. The increased risk
continued to be significant after controlling for obesity and
diabetes, which was consistent with the hypothesis that these
variables would act as partial mediators. Short sleep duration
could, therefore, be a significant risk factor for hypertension.”
|
314
|
|
Go
to TOC
Vitamins,
minerals, supplements and spices
Other
possible supplements
I
simply do not have enough reliable information on these things to
comment much, but they look promising based on various claims. I
await better studies.
Metformin
(antidiabetic drug) has been shown to substantially increase lifespan
in rodent models, an average of 21%!
Hormone replacement
therapy for those older than age 50 (natural production of hormones
such as melatonin, growth hormone, sex hormones, etc. decline
dramatically at about this age, possibly with detrimental effects).
Unfortunately hormone replacement may also increase the rates of
aging and cancer (such as prostate cancer). I think this is likely to
be a BAD idea in all cases I know of.
A
combination of R(+) alpha lipoic acid and acetyl-L-carnitine that
appears to simultaneously increase energy (“youthfulness”) in
rats, and act as a potent antioxidant where it counts – the
mitochondria. The former helps you feel better as you age, the latter
may help slow the aging process. Sounds “too good to be true”,
but has the positive signs of support by the NIH, and research done
at UC Berkeley. These positive effects have been confirmed
anecdotally in people; a high-quality clinical trial is currently
under way. Racemic alpha lipoic acid is currently available as a
dietary supplement “Juvenon” – at a cost: $39.95 + S&H. I
have started taking this myself… Note: the racemic alpha lipoic
acid is a mixture of R and S enantiomers (mirror-images); the R form
is active, the S form is at best inactive, and at worst harmful.
Articles supporting R(+) alpha lipoic acid are: (FASEB
J 1998 Sep;12(12):1183-9; PMID 9737721,
FASEB
J 1999 Feb;13(2):411-8 ; PMID 9973329, Antioxid
Redox Signal 2000 Fall;2(3):473-83 ; PMID 11229361,
FASEB
J 2001 Mar;15(3):700-6 ; PMID 11259388, Proc
Natl Acad Sci U S A 2002 Feb 19;99(4):1870-5; PMID 11854487,
Proc
Natl Acad Sci U S A 2002 Feb 19;99(4):1876-81; PMID 11854488,
Proc
Natl Acad Sci U S A 2002 Feb 19;99(4):2356-61; PMID 11854529,
Hagen
TM, Moreau R, Suh JH, Visioli F. Mitochondrial decay in the aging rat
heart: evidence for improvement by dietary supplementation with
acetyl-L-carnitine and/or lipoic acid. Ann N Y Acad Sci. 2002
Apr;959:491-507. Review. PMID: 11976222; Hagen
TM, Liu J, Lykkesfeldt J, Wehr CM, Ingersoll RT, Vinarsky V,
Bartholomew JC, Ames BN. Feeding acetyl-L-carnitine and lipoic acid
to old rats significantly improves metabolic function while
decreasing oxidative stress. Proc Natl Acad Sci U S A. 2002 Feb
19;99(4):1870-5. PMID: 11854487).
Creatine
seems to improve brain function as well as sports performance. “we
tested the hypothesis that oral creatine supplementation (5 g d(-1)
for six weeks) would enhance intelligence test scores and working
memory performance in 45 young adult, vegetarian subjects in a
double-blind, placebo-controlled, cross-over design. Creatine
supplementation had a significant positive effect (p < 0.0001) on
both working memory (backward digit span) and intelligence (Raven's
Advanced Progressive Matrices), both tasks that require speed of
processing. These findings underline a dynamic and significant role
of brain energy capacity in influencing brain performance.”
(Rae C, Digney AL, McEwan SR, Bates TC. Oral creatine
monohydrate supplementation improves brain performance: a
double-blind, placebo-controlled, cross-over trial. Proc R Soc Lond B
Biol Sci. 2003 Oct 22;270(1529):2147-50. PMID:
14561278)
See
also homocysteine.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Recommended
vitamin doses
|
|
This web site has
a list. “The Dietary Reference Intakes (DRI) are the most recent
set of dietary recommendations established by the Food and
Nutrition Board of the Institute of Medicine, 1997-2001. They
replace previous RDAs”
|
315
|
|
|
Folate
|
Reduces
colon cancer risk by 40%
|
“Epidemiologic
and clinical studies indicate that dietary folate intake and
blood folate levels are inversely associated with colorectal
cancer risk. Collectively, these studies suggest an
40%
reduction in the risk of colorectal cancer in
individuals with the highest dietary folate intake
compared with those with the lowest intake.”
|
316
|
|
|
|
Strongly
associated with reduced dementia
|
A
study of 228 subjects found that low folate levels or high
homocysteine levels were strongly associated with mild cognitive
development, vascular dementia, and Alzheimer disease.
(approximately 3-fold increased risk)
|
317
|
|
|
|
Associated
with decreased risk of HTN
|
“younger
women who consumed at least 1000 microg/d of total folate (dietary
plus supplemental) had a decreased risk of hypertension”
|
318
|
|
|
|
Dose-response
reduction in homocysteine. Maximum effect is at about 0.8 mg
|
“daily
doses of 0.2, 0.4, 0.8, 2.0, and 5.0 mg folic acid were associated
with reductions in homocysteine of 13% (95% CI: 10%, 16%), 20%
(17%, 22%), 23% (21%, 26%), 23% (20%, 26%), and 25% (22%, 28%),
respectively. Vitamin B-12 (x: 0.4 mg/d) produced 7% (95% CI: 4%,
9%) further reduction in homocysteine concentrations, but vitamin
B-6 had no significant effect.”
|
319
|
|
|
Folate
and B12
|
Older
people need them
|
“…significant
vitamin B12 deficiency increased with age in all three studies,
from about 1 in 20 among people aged 65-74 years to 1 in 10 or
even greater among people aged 75 years or greater. The prevalence
of folate deficiency also increased with age, and was similar to
that for vitamin B12 deficiencies…”
|
320
|
|
|
Vitamin
D
|
Supplements
help vs osteoporosis
|
“Relative
risk of falling in the groups supplemented with vitamin D was 0.48
(95% CI 0.26-0.90) compared with controls. CONCLUSION: Vitamin D
supplementation, either orally or with injected vitamin D,
suppresses parathyroid hormone, increases bone mineral density and
reduces falls.” [Note from other sources: exercise also helps;
calcium supplements and milk may not.]
|
321
|
|
|
|
Take
cholecalciferol (D3), NOT ergocalciferol (D2)
|
“vitamin
D(3) [chlecalciferol] has proven to be the more potent form of
vitamin D in all primate species, including humans…the form of
vitamin D used in major preparations of prescriptions in North
America is vitamin D(2)…Vitamin D(2), or ergocalciferol, should
not be regarded as a nutrient suitable for supplementation or
fortification.”
|
322
|
|
|
|
May
help prevent multiple sclerosis (MS)
|
This
could explain the long-observed fact that those who grow up in
northern areas tend to have a higher incidence of MS. “Intake of
vitamin D from supplements was also inversely associated with risk
of MS; the RR comparing women with intake of >or=400 IU/day
with women with no supplemental vitamin D intake was 0.59 (95% CI
= 0.38 to 0.91; p for trend = 0.006). No association was found
between vitamin D from food and MS incidence.”
|
323
|
|
|
|
|
“Prospective,
nested case-control study among more than 7 million US military
personnel who have serum samples stored in the Department of
Defense Serum Repository. Multiple sclerosis cases were identified
through Army and Navy physical disability databases for 1992
through 2004, and diagnoses were confirmed by medical record
review. Each case (n = 257) was matched to 2 controls by age, sex,
race/ethnicity, and dates of blood collection. Vitamin D status
was estimated by averaging 25-hydroxyvitamin D levels of 2 or more
serum samples collected before the date of initial multiple
sclerosis symptoms. MAIN OUTCOME MEASURES: Odds ratios of multiple
sclerosis associated with continuous or categorical levels
(quantiles or a priori-defined categories) of serum
25-hydroxyvitamin D within each racial/ethnic group. RESULTS:
Among whites (148 cases, 296 controls), the risk of multiple
sclerosis significantly decreased with increasing levels of
25-hydroxyvitamin D (odds ratio [OR] for a 50-nmol/L increase in
25-hydroxyvitamin D, 0.59; 95% confidence interval,
0.36-0.97). In categorical analyses using the lowest quintile
(<63.3 nmol/L) as the reference, the ORs for each subsequent
quintile were 0.57, 0.57, 0.74, and 0.38 (P = .02 for trend across
quintiles). Only the OR for the highest quintile, corresponding to
25-hydroxyvitamin D levels higher than 99.1 nmol/L, was
significantly different from 1.00 (OR, 0.38; 95% confidence
interval, 0.19-0.75; P = .006). The inverse relation with
multiple sclerosis risk was particularly strong for
25-hydroxyvitamin D levels measured before age 20 years…The
results of our study suggest that high circulating levels of
vitamin D are associated with a lower risk of multiple sclerosis.”
|
324
|
|
|
|
You
should take MORE than the RDA
|
“The
recommended adequate intakes for vitamin D are inadequate,
and, in the absence of exposure to sunlight, a minimum of
1000 IU vitamin D/d is required to maintain a healthy
concentration of 25(OH)D in the blood.”
|
325
|
|
|
|
The
upper limit of vitamin D intake should be no less than 10,000
IU per day
|
“Except
in those with conditions causing hypersensitivity, there is no
evidence of adverse effects with serum 25(OH)D concentrations <140
nmol/L, which require a total vitamin D supply of 250 microg
(10000 IU)/d to attain. Published cases of vitamin D toxicity with
hypercalcemia, for which the 25(OH)D concentration and vitamin D
dose are known, all involve intake of > or = 1000 microg (40000
IU)/d. Because vitamin D is potentially toxic, intake of >25
microg (1000 IU)/d has been avoided even though the weight of
evidence shows that the currently accepted, no observed adverse
effect limit of 50 microg (2000 IU)/d is too low by at least
5-fold.”
|
326
|
|
|
|
May
help prevent some cancers
|
“Inverse
correlations are found for UV-B radiation for a number of cancers,
with those for bladder, breast, endometrial, ovarian, prostate,
and renal cancer, and multiple myeloma and NHL having the
strongest correlations in this and ongoing multicountry ecologic
studies. These studies add further support for the role of UV-B
radiation and vitamin D in reducing the risk of a large number of
cancers.”
|
327
|
|
|
|
|
“daily
intake of 1,000 international units (IU) or 25 micrograms(μg) of
vitamin D3 may lower the risk of developing colon, breast,
prostate and ovarian cancers by up to 50 percent…Vitamin
D supplements may be needed to supplement dietary sources of
vitamin D, which are likely not enough to provide 1,000 IU daily
recommended by the researchers of the current study.
One glass of milk may offer only 100 IU of
vitamin D.”
“Vitamin
D status differs by latitude and race, with residents of the
northeastern United States and individuals with more skin
pigmentation being at increased risk of deficiency. A PubMed
database search yielded 63 observational studies of vitamin D
status in relation to cancer risk, including 30 of colon,
13 of breast, 26 of prostate, and 7 of ovarian
cancer, and several that assessed the association of vitamin D
receptor genotype with cancer risk. The majority of studies found
a protective relationship between sufficient vitamin D status and
lower risk of cancer. The evidence suggests that efforts to
improve vitamin D status, for example by vitamin D
supplementation, could reduce cancer incidence and mortality at
low cost, with few or no adverse effects.”
|
328
329
|
|
|
|
May
help prevent periodontal disease
|
A
study of 11,202 subjects found that for those >50 yr of age,
“Compared with men in the highest 25(OH)D3
[vitamin D] quintile, those in the lowest quintile had
a mean [periodontal attachment loss] that was 0.39 mm (95% CI:
0.17, 0.60 mm) higher; in women, the difference in
[periodontal attachment loss] between the lowest and highest
quintiles was 0.26 mm (0.09, 0.43 mm).”
|
330
|
|
|
|
May
help prevent infection
|
Detailed
in a summary article in Science News
|
331
|
|
|
|
Good
summary article
|
From
Science News. The messages: Vitamin D helps prevent muscle
problems, immune problems, etc. and you need to take much more
vitamin D than the RDA.
|
332
|
|
|
|
Made
on sun exposure
|
From Wikipedia,
“At higher latitudes, total vitamin D input from sunlight is
usually insufficient, especially in the winter.” “Vitamin
D3... is derived from animal sources and is made in the
skin when 7-dehydrocholesterol reacts with UVB ultraviolet light
with wavelengths 290 to 315 nm. These wavelengths are
present in sunlight at sea level when the sun is more than 45°
above the horizon, or when the UV index is greater than 3.”
Note:
the best way to get enough vitamin D3 is from (cheap) supplements,
because UV exposure (sunlight) results in skin cancers.
|
|
|
|
Vitamins
C & E
|
Associated
with reduced Alzheimer Disease risk
|
A
cross-sectional, prospective study from Utah of 4740 people >
64 yr. old found that “Use of vitamin E and C (ascorbic acid)
supplements in combination was associated with reduced AD
prevalence (adjusted odds ratio, 0.22; 95% confidence interval,
0.05-0.60) and incidence (adjusted hazard ratio, 0.36; 95%
confidence interval, 0.09-0.99). A trend toward lower AD risk was
also evident in users of vitamin E and multivitamins containing
vitamin C, but we saw no evidence of a protective effect with use
of vitamin E or vitamin C supplements alone, with multivitamins
alone, or with vitamin B-complex supplements.”
|
333
|
|
|
Vitamin
E (alpha-tocopherol)
|
Does
NOT help prevent heart disease
|
“…strong
support for a lack of statistically significant or clinically
important effects of vitamin E on cardiovascular disease.”
|
334
|
|
|
|
Associated
with HIGHER all-cause mortality
|
“PURPOSE:
To perform a meta-analysis of the dose-response relationship
between vitamin E supplementation and total mortality by using
data from randomized, controlled trials. PATIENTS: 135,967
participants in 19 clinical trials… A dose-response analysis
showed a statistically significant relationship between vitamin E
dosage and all-cause mortality, with increased risk of dosages
greater than 150 IU/d… CONCLUSION: High-dosage (> or =400
IU/d) vitamin E supplements may increase all-cause mortality and
should be avoided.”
|
335
|
|
|
Iron
|
Too
low an iron level is bad
|
Very
low iron levels (iron deficiency) causes increased mitochondrial
oxidation => accelerated aging and neural decay.
|
336
|
|
|
|
Iron
supplements may possibly cause intestinal damage
|
An 80 mg iron
dose study found “These data show that a single dosage of
ferrous sulfate induces oxidative damage … in the small
intestine in vivo in healthy volunteers.”
Review
of iron’s effects on the bowel
|
337
338
|
|
|
Acetyl-L-carnitine
|
May
reduce age-related changes in brain lipids
|
“…changes
in membrane lipid metabolism and/or composition represent one of
the alterations occurring in rat brain with aging, and that
long-term feeding with acetyl-L-carnitine can be useful in
normalizing these age-dependent disturbances.”
|
339
|
|
|
Curcumin
|
Should
be eaten with pepper
|
The
possibly beneficial compound curcumin is found in the spice
turmeric. However, it is almost completely metabolized by the
intestine and liver by glucuronidation. Piperine found in peppers
inhibits this metabolism. “Concomitant administration of
piperine 20 mg produced much higher concentrations from 0.25 to 1
h post drug (P < 0.01 at 0.25 and 0.5 h; P < 0.001 at 1 h),
the increase in bioavailability was 2000%.” Peppers have about
6% piperine, which accounts for its pungent flavor (see
http://www-ang.kfunigraz.ac.at/~katzer/engl/generic_frame.html?Curc_lon.html).
Turmeric has about 4% curcumin
(http://www-ang.kfunigraz.ac.at/~katzer/engl/generic_frame.html?Curc_lon.html).
|
340
|
|
|
|
Associated
with lesser cognitive decline
|
“The
authors investigated the association between usual curry
consumption level and cognitive function in elderly Asians. In a
population-based cohort (n = 1,010) of nondemented elderly Asian
subjects aged 60-93 years in 2003, the authors compared
Mini-Mental State Examination (MMSE) scores for three categories
of regular curry consumption…Those who consumed curry
"occasionally" and "often or very often" had
significantly better MMSE scores than did subjects who "never
or rarely" consumed curry.”
|
341
|
|
|
Calcium
|
Associated
with lower rate of colon cancer
|
“After
adjustment for known risk factors, adenoma risk was
lower by 12% for participants in the highest quintile of
total calcium intake (>1767 mg/d) than for participants
in the lowest quintile (<731 mg/d) (odds ratio:
0.88; 95% CI: 0.76, 1.02; P for trend = 0.04).
The protective association between total calcium and
colorectal adenoma was largely due to calcium
supplement use, with a 27% decrease in adenoma risk for
participants taking >1200 mg/d than for nonusers of supplements
(odds ratio: 0.73; 95% CI: 0.56, 0.91; P for trend =
0.005).”
|
342
|
|
|
|
Lower
rate of stroke and death
|
“The
multivariate relative risk for men with highest versus lowest
quintiles of dairy calcium intake was 0.53 (95% CI, 0.34 to 0.81)
for total stroke, 0.46 (0.23 to 0.91) for hemorrhagic stroke, and
0.53 (0.29 to 0.99) for ischemic stroke; corresponding relative
risks for women were 0.57 (0.38 to 0.86), 0.51 (0.28 to 0.94), and
0.50 (0.27 to 0.95). CONCLUSIONS: Dietary calcium intake from
dairy products was associated with reduced mortality from stroke
for Japanese men and women.”
|
343
|
|
|
Magnesium
|
High
intake associated with 33% lower rate of diabetes type 2
|
“We
followed 85,060 women and 42,872 men who had no history of
diabetes… After 18 years of follow-up in women and 12 years in
men… After adjusting for age, BMI, physical activity, family
history of diabetes, smoking, alcohol consumption, and history of
hypertension and hypercholesterolemia at baseline, the relative
risk (RR) of type 2 diabetes was 0.66 (95% CI 0.60-0.73; P for
trend <0.001) in women and 0.67 (0.56-0.80; P for trend <0.001)
in men, comparing the highest with the lowest quintile of total
magnesium intake… This study supports the dietary
recommendation to increase consumption of major food sources of
magnesium, such as whole grains, nuts, and green leafy
vegetables.”
|
344
|
|
|
|
Sources
of magnesium345
|
Source
Serving
Magnesium
(mg)
100%
Bran Cereal (e.g. All Bran)
1/2
cup
128.7
Spinach,
chopped
1/2
cup cooked
78.3
Almonds
1
ounce
81.1
Oat
bran
1/2
cup dry
96.4
|
|
|
|
|
Associated
with a lower rate of colon cancer (in dietary sources)
|
“a
population-based prospective cohort of 61,433 women aged 40 to 75
years without previous diagnosis of cancer at baseline from 1987
to 1990… During a mean of 14.8 years (911 042 person-years) of
follow-up, 805 incident colorectal cancer cases were diagnosed.
After adjustment for potential confounders, we observed an inverse
association of magnesium intake with the risk of colorectal cancer
(P for trend = .006). Compared with women in the lowest quintile
of magnesium intake, the multivariate rate ratio (RR) was 0.59
(95% confidence interval [CI], 0.40-0.87) for those in the highest
quintile. The inverse association was observed for both colon (RR,
0.66; 95% CI, 0.41-1.07) and rectal cancer (RR, 0.45;
95% CI, 0.22-0.89).”
|
346
|
|
|
|
|
“a
cohort of 35,196 Iowa women initially free of cancer and aged
55-69 years in 1986. Intakes of magnesium and other nutrients were
assessed by food frequency questionnaire at baseline. Over 17
years of follow-up through 2002, 1,112 women developed colorectal
cancer. After adjustment for age, energy, other nutrients, and
risk factors for colorectal cancer, the hazard ratios of
colorectal cancer across quintiles of magnesium intake were 1.00,
0.96, 0.83, 0.87, and 0.80 (95% confidence interval: 0.62, 1.03;
ptrend = 0.06). The association was largely absent for rectal
cancer but, for colon cancer, the hazard ratios were 1.00, 1.00,
0.88, 0.85, and 0.77 (95% confidence interval: 0.58, 1.03; ptrend
= 0.04). These findings offer further evidence that a diet high in
magnesium may reduce the occurrence of colon cancer among women.”
|
347
|
|
|
|
Associated
with better muscle function in the elderly
|
“From
among 1453 randomly selected community residents completing a home
interview, 1138 men (46%) and women (aged 66.7 ± 15.2 y;
 ±
SD) with complete data on muscle performance and serum magnesium
who were not severely cognitively compromised … were included in
the analysis. Muscle performance was evaluated by grip strength,
lower-leg muscle power, knee extension torque, and ankle extension
isometric strength and was normalized for age and body mass index
(BMI) within each sex. Results: After adjustment for age, sex,
BMI, laboratory variables, presence of chronic diseases, muscle
area, muscle density, and physical activity level, serum
magnesium concentrations were significantly associated with
indexes of muscle performance, including grip strength …,
lower-leg muscle …, knee extension torque …, and ankle
extension strength” ±
SD) with complete data on muscle performance and serum magnesium
who were not severely cognitively compromised … were included in
the analysis. Muscle performance was evaluated by grip strength,
lower-leg muscle power, knee extension torque, and ankle extension
isometric strength and was normalized for age and body mass index
(BMI) within each sex. Results: After adjustment for age, sex,
BMI, laboratory variables, presence of chronic diseases, muscle
area, muscle density, and physical activity level, serum
magnesium concentrations were significantly associated with
indexes of muscle performance, including grip strength …,
lower-leg muscle …, knee extension torque …, and ankle
extension strength”
|
348
|
|
|
|
Associated
with lesser severity of asthma
|
“37
patients (aged 7-19 years, 19 males) were randomized in two
groups: magnesium (n=18, 300 mg/day) and placebo (n=19), during 2
months. …The primary outcome was bronchial reactivity…The
magnesium group presented fewer asthma exacerbations and used less
salbutamol compared to the placebo group. Conclusions: Oral
magnesium supplementation helped to reduce bronchial reactivity
to methacholine, to diminish their allergen-induced skin responses
and to provide better symptom control in pediatric patients with
moderate persistent asthma treated with inhaled fluticasone.”
|
349
|
|
|
Selenium
|
May
help reduce the risk of prostate cancer
|
“A
large body of epidemiological evidence, including observational,
case-control, cohort and randomized controlled clinical trials,
support the proposition that selenium may prevent prostate cancer
in humans.”
|
350
|
|
|
Benfotiamine
(a niacin derivative, available as a supplement)
|
Helps
prevent glucose damage to the retina
|
“Three
of the major biochemical pathways implicated in the pathogenesis
of hyperglycemia induced vascular damage (the hexosamine pathway,
the advanced glycation end product (AGE) formation pathway and the
diacylglycerol (DAG)-protein kinase C (PKC) pathway) are activated
by increased availability of the glycolytic metabolites
glyceraldehyde-3-phosphate and fructose-6-phosphate. We have
discovered that the lipid-soluble thiamine derivative benfotiamine
can inhibit these three pathways, as well as
hyperglycemia-associated NF-kappaB activation, by activating the
pentose phosphate pathway enzyme transketolase, which converts
glyceraldehyde-3-phosphate and fructose-6-phosphate into
pentose-5-phosphates and other sugars. In retinas of diabetic
animals, benfotiamine treatment inhibited these three pathways and
NF-kappaB activation by activating transketolase, and also
prevented experimental diabetic retinopathy. The ability of
benfotiamine to inhibit three major pathways simultaneously might
be clinically useful in preventing the development and progression
of diabetic complications.”
|
351
|
|
|
|
Helps
prevent damage from glucose (AGEs, diabetes)
|
Benfotiamine
helps prevent diabetic nephropathy (kidney disease)
|
352
|
|
|
Make
sure your nutrition is adequate
|
CR
mice live longer with optimal diet
|
Six
groups of mice were studied with variations in diet quality
(standard diet vs. enriched for protein, vitamins and minerals)
and % CR. The CR mice survived longer than the ad lib mice; the CR
+ optimal diet survived longest of all and were healthiest.
|
353
|
|
|
B12
|
Helps
prevent osteoporosis
|
From
the Framingham Offspring Osteoporosis Study (1996-2001): “Both
men and women with vitamin B12 concentrations <148 pM had lower
average BMD than those with vitamin B12 above this cut-off. These
differences were significant (p < 0.05) for men at most hip
sites and for women at the spine.”
|
354
|
|
|
|
Deficiency
is common in the elderly
|
“This
was a cross-sectional survey of 84 nondemented elderly
participants (aged >69 y) from the Welsh cohort…Nearly
one-half (43%) of the persons selected had likely metabolically
significant vitamin B-12 deficiency.” And this was associated
with decreased mental function.
|
355
|
|
|
Calcium
|
May
NOT prevent osteoporosis
|
|
356
|
|
|
Beta
carotene, vitamins C and E, and zinc
|
|
“Dietary
intake was assessed at baseline in the Rotterdam Study (1990-1993)
using a semiquantitative food frequency questionnaire. Incident
AMD until final follow-up in 2004 was determined by grading fundus
color transparencies in a masked way according to the
International Classification and Grading System. SETTING:
Population-based cohort of all inhabitants aged 55 years or older
in a middle-class suburb of Rotterdam, the Netherlands.
PARTICIPANTS: Of 5836 persons at risk of AMD at baseline, 4765 had
reliable dietary data and 4170 participated in the follow-up. MAIN
OUTCOME MEASURE: Incident AMD, defined as soft distinct drusen
with pigment alterations, indistinct or reticular drusen,
geographic atrophy, or choroidal neovascularization. RESULTS:
Incident AMD occurred in 560 participants after a mean follow-up
of 8.0 years (range, 0.3-13.9 years). Dietary intake of both
vitamin E and zinc was inversely associated with incident AMD. The
hazard ratio (HR) per standard deviation increase of intake for
vitamin E was 0.92 (95% confidence interval [CI], 0.84-1.00) and
for zinc was 0.91 (95% CI, 0.83-0.98). An above-median intake of
all 4 nutrients, beta carotene, vitamin C, vitamin E, and zinc,
was associated with a 35% reduced risk (HR, 0.65; 95% CI,
0.46-0.92) of AMD. Exclusion of supplement users did not affect
the results. CONCLUSION: In this study, a high dietary intake of
beta carotene, vitamins C and E, and zinc was associated with a
substantially reduced risk of AMD in elderly persons.”
|
357
|
|
Go
to TOC
General
and Broad recommendations
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Overall
diet recommendations vs. coronary heart disease (CHD)
|
Cut
some fats
Increase
intake of whole grains, omega-3 fats, fruit and vegetables
|
“Compelling
evidence from metabolic studies, prospective cohort
studies, and clinical trials in the past several decades indicates
that at least 3 dietary strategies are effective in preventing
CHD: substitute nonhydrogenated unsaturated fats for saturated and
trans-fats; increase consumption of omega-3 fatty acids from fish,
fish oil supplements, or plant sources; and consume a diet high in
fruits, vegetables, nuts, and whole grains and low in refined
grain products. … Substantial evidence indicates that diets
using nonhydrogenated unsaturated fats as the predominant form of
dietary fat, whole grains as the main form of carbohydrates, an
abundance of fruits and vegetables, and adequate omega-3 fatty
acids can offer significant protection against CHD. Such diets,
together with regular physical activity, avoidance of smoking, and
maintenance of a healthy body weight, may prevent
the majority of cardiovascular disease in Western populations.”
|
358
|
|
|
Fats
and carbohydrates
|
Altering
fat and carbohydrate intake works better than medicine to reduce
cardiovascular disease risk factors
|
A
thorough review of the literature to date. Among other things:
1.
Diet works better than medicine: “The reductions in
cardiovascular disease (CVD) caused by these dietary therapies
compare favorably with drug treatments for hyperlipidemia and
hypertension.”
2. “The n-3 polyunsaturated fats in fish
oils suppress cardiac arrhythmias and reduce triglycerides, but
they have little effect on LDL or HDL cholesterol levels.”
3.
“…triglycerides increase … when carbohydrate increases,
except when low glycemic index foods are used.”
|
359
|
|
|
|
|
“Diets
higher in MUFA, higher in fiber with a low glycemic index continue
to show advantages in reducing risk and risk factors for chronic
disease, especially those associated with insulin resistance. The
simple classification of diets into high-fat versus
high-carbohydrate appears less helpful in predicting the metabolic
outcome.”
|
360
|
|
|
Food
pyramid
|
Revised
based on modern nutritional understanding
|
Base
of pyramid is whole grains, specific vegetable oils, vegetables,
fruit and nuts! This is worth looking at on line (see the
reference).
|
361
|
|
|
Breakfast
|
|
One study looked
at the breakfast habits of "...262 volunteers aged between 21
and 85 years, mean age: 60.9 years... The results showed that
those who consumed breakfast cereal every day reported better
mental and physical health than those who consumed it less
frequently. This association was still present when demographic
factors [including] other aspects of diet were covaried."
Another study
evaluated the effects of breakfast and coffee on 142 volunteers.
“…The results showed that those who consumed breakfast cereal
had a more positive mood at the start of the test sessions,
performed better on a spatial memory task, and felt calmer at the
end of the test session than those in the no breakfast condition.
Ingestion of caffeine had no effect on initial mood or working
memory, but it did improve encoding of new information and
counteracted the fatigue that developed over the test session.
Caffeine increased blood pressure and pulse rate, whereas
breakfast cereal consumption only had an effect on pulse.”
A meta-analysis
of three studies (not including the above two studies) concluded
that breakfast improves memory-task performance.
“[Omitting
breakfast] impairs fasting lipids and postprandial insulin
sensitivity and could lead to weight gain if the observed higher
energy intake was sustained.”
|
362
363
364
365
|
|
|
Protein
|
Vegetable
protein in large amounts may help vs. HTN and heart disease
|
“Recent
evidence suggests that an increased intake of protein,
particularly plant protein, may lower blood pressure and reduce
the risk of cardiovascular disease. However, the data are not
sufficiently compelling to advocate an increased consumption of
protein.”
|
366
|
|
Go
to TOC
Toxins
and carcinogens
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Iron
and manganese
|
Associated
with increased risk of Parkinson Disease
|
“Subjects
with an iron intake in the highest quartile compared with those in
the lowest quartile had an increased risk of PD (odds ratio = 1.7,
95% CI: 1.0, 2.7, trend p = 0.016). There was an apparent joint
effect of iron and manganese; dietary intake above median levels
of both together conferred a nearly doubled risk compared with
lower intakes of each nutrient (odds ratio = 1.9…”
|
367
|
|
|
Iron
|
Supplements
damage the GI tract
|
A
review discusses the toxic effects of iron supplements,
particularly when taken with vitamin C. “Co-supplementation of
ferrous salts with vitamin C exacerbates oxidative stress in the
gastrointestinal tract, predisposing individuals to ulceration,
inflammatory disorders, and exacerbation of existing chronic
disorders and may cause cancer.”
|
368
|
|
|
Mercury
|
Even
LOW LEVEL exposure in ADULTS affects neurologic performance
|
“The
strongest effects of mercury on persons in this study were
detected on tests of fine motor speed and dexterity (Bead
Threading) and response inhibition (errors of commission or "false
alarms" on the timed visual search and attention tasks). The
size of the effects increased with hair mercury concentration,
consistent with a dose-dependent effect…the public health
impacts of MeHg exposure at levels often encountered by adults in
North America [2]
may be inducing adverse effects on neurobehavioral performance.”
|
369
|
|
|
Polycyclic
aromatic hydrocarbons (PAH)
|
Smoke
flavor has small amounts of PAH and is safer than grilling
|
“…the
flavoring obtained from poplar wood presents the highest number
and concentrations of both total and carcinogenic PAHs, even
though the levels of these latter are very low.”
|
370
|
|
|
|
How
to reduce PAHs from grilling
|
From
AICR: Best, do not grill!
Also:
pre-heat the meat, use sauces and marinades for flavor, use
low-fat meat, grill far from hot coals or flames.
|
371
372
|
|
|
Risk
factors for Parkinson Disease
|
Lead
& copper, insecticide, family history, smoking
|
A
“health system population-based case-control study of
epidemiological risk factors” found that “>20 years joint
occupational exposure to lead and copper (p=0.009; population
attributable risk [PAR]=3.9%), occupational exposure to
insecticides (p=0.002; PAR=8.1%), a positive family history of PD
in first- and second-degree relatives (p=0.001; PAR=12.4%), and
smoking </=30 pack-years or not smoking (p=0.005; PAR=41.4%).”
Altogether these could account for 54% of Parkinson Disease.
|
373
|
|
|
Aluminum
|
May
cause Alzheimer Disease (n.b., there is very limited epidemiologic
evidence)
|
“Aluminum
(Al) has been etiologically and epidemiologically related to
several neurologic conditions, including Alzheimer's disease
(AD).” In rats, chronic high dose aluminum exposure, “The
experimental animals had impaired spatial memory, with lower and
more fluctuant performance at Morris water maze…The brains of
experimental animals, studied by optical microscopy, displayed a
massive cellular depletion in the hippocampal formation, …The
hippocampus contained extracellular accumulations of Al and
amyloid … These behavioral and neuropathological modifications
associated with long-term exposure to Al are reminiscent of those
observed in AD.”
|
374
|
|
|
Aluminum
and Fluoride
|
High
concentration in tea, may cause toxic accumulations
|
“Tea
plant takes up a large quantity of aluminium (Al) and fluoride (F)
from acidic soils. It has been known that fluorosis can be
developed for people who consume a large quantity of tea made from
brick tea, a low quality tea consisting mainly of old tea leaves
in China.”
|
375
|
|
|
Pesticides
|
Some
fruit and vegetables have more than others
I
personally think this does not matter much compared to other
factors
|
See
the table at http://www.foodnews.org/reportcard.php
12
Most Contaminated
.
Apples
.
Bell Peppers
.
Celery
.
Cherries
.
Imported Grapes
.
Nectarines
.
Peaches
.
Pears
.
Potatoes
.
Red Raspberries
.
Spinach
.
Strawberries
12
Least Contaminated
.
Asparagus
.
Avocados
.
Bananas
.
Broccoli
.
Cauliflower
.
Corn (sweet)
.
Kiwi
.
Mangos
.
Onions
.
Papaya
.
Pineapples
.
Peas (sweet)
|
|
|
|
Soy
|
May
(very limited evidence) be associated with cognitive decline
|
“Poor
cognitive test performance, enlargement of ventricles and low
brain weight were each significantly and independently associated
with higher midlife tofu consumption…Odds ratios comparing
endpoints among "high-high" with "low-low"
consumers were mostly in the range of 1.6 to 2.0.”
|
376
|
|
|
|
Worsens
heart disease in a mouse model that may or may not be relevant to
humans
|
“We
report that dietary modification from a soy-based diet to a
casein-based diet radically improves disease indicators and
cardiac function in a transgenic mouse model of hypertrophic
cardiomyopathy. On a soy diet, males with a mutation in the
alpha-myosin heavy chain gene progress to dilation and heart
failure. However, males fed a casein diet no longer deteriorate to
severe, dilated cardiomyopathy.”
|
377
|
|
|
Vitamin
E (alpha-tocopherol)
|
Associated
with HIGHER all-cause mortality
|
“PURPOSE:
To perform a meta-analysis of the dose-response relationship
between vitamin E supplementation and total mortality by using
data from randomized, controlled trials. PATIENTS: 135,967
participants in 19 clinical trials… A dose-response analysis
showed a statistically significant relationship between vitamin E
dosage and all-cause mortality, with increased risk of dosages
greater than 150 IU/d… CONCLUSION: High-dosage (> or =400
IU/d) vitamin E supplements may increase all-cause mortality and
should be avoided.”
|
378
|
|
|
Lead
|
Is
at a high level in chocolate
|
“lead
concentrations of manufactured cocoa and chocolate products were
as high as 230 and 70 ng/g, respectively, which are consistent
with market-basket surveys that have repeatedly listed lead
concentrations in chocolate products among the highest reported
for all foods. One source of contamination of the finished
products is tentatively attributed to atmospheric emissions of
leaded gasoline, which is still being used in Nigeria. Because of
the high capacity of cocoa bean shells to adsorb lead,
contamination from leaded gasoline emissions may occur during the
fermentation and sun-drying of unshelled beans at cocoa farms.”
Equal
Exchange sources their cocoa from cooperatives in the Dominican
Republic, where leaded gasoline has been totally banned since
1999, so the lead issue SHOULD be largely obviated.
|
379
380
|
|
|
Air
pollution
|
Correlated
with high risk of heart attack
|
Perhaps
fine particulates. “The findings of the study support the
hypothesis that particles can induce cardiovascular disease
through inflammatory pathways, suggestive of a greater toxicity of
traffic-related particles.”
|
381
|
|
|
Copper
|
Associated
with late-life mental decline, when in association with trans or
saturated fats
|
Multi-vitamins
often have 2 mg of copper; this may be one of the causes of mental
decline or Alzheimer Disease. Those with the highest copper and
bad fat intake added the equivalent of 19 years to their ages in
terms of mental decline.
“Evidence
from prospective epidemiologic studies and animal models suggests
that intakes of dietary fats and copper may be associated with
neurodegenerative diseases… Among persons whose diets were
high in saturated and trans fats, higher copper intake was
associated with a faster rate of cognitive decline. In
multiple-adjusted mixed models, the difference in rates for
persons in the highest (median, 2.75 mg/d) vs lowest (median, 0.88
mg/d) quintiles of total copper intake was -6.14 standardized
units per year (P<.001) or the equivalent of 19 more years of
age. There was also a marginally statistically significant
association (P = .07) with the highest quintile of food intake of
copper (median, 1.51 mg/d) and a strong dose-response
association with higher copper dose in vitamin supplements. Copper
intake was not associated with cognitive change among persons
whose diets were not high in these fats.”
|
382
|
|
|
|
Associated
with higher death rate
|
“Data
from the Paris Prospective Study 2, a cohort of 4035 men age 30-60
years at baseline, were used to assess the association between
serum zinc, copper, and magnesium and all-cause, cancer, and
cardiovascular disease mortality…During 18-year follow up, 339
deaths occurred, 176 as a result of cancer and 56 of
cardiovascular origin. Relative risks (RRs) for each element were
inferred using Cox's proportional hazard model after controlling
for various potential confounders. RESULTS: High copper values
(4th quartile) were associated with a 50% increase in RRs for
all-cause deaths …High magnesium values were negatively
related to mortality with a 40% decrease in RR for all-cause”
|
383
|
|
|
Cinnamon
|
Contains
coumarin
|
Coumarin
(also used in rat poison) can cause cancer and liver damage. The
levels of coumarin in cinnamon can be very high. A little on
applesauce is OK, but large quantities are not.
“Ceylon
cinnamon” has substantially lower levels of coumarin than cassia
or Chinese cinnamon (1/10th).
|
384
|
|
|
Stevia
|
|
“In
one of the rat studies (14), a 13-week dose-finding study, cell
necrosis in the liver of all treated males was reported (lowest
dose equivalent to 155 mg/kg bw) ”
|
385
|
|
Cholesterol
Go
to TOC
Ultraviolet
light
Get
out of the sun, and use maximum sun block (SPF 45 to 50) if you have
to be out in the sun. The
sun block should be broad spectrum, protecting well against both UVA
and UVB; microfine / micronized
zinc oxide is perhaps the best. UVB is far more damaging than UVA,
but there is far more UVA from the sun. UVA exposure has been shown
to damage mitochondria, in effect hastening aging (Koch
H, Wittern KP, Bergemann J. In human keratinocytes the Common
Deletion reflects donor variabilities rather than chronologic aging
and can be induced by ultraviolet A irradiation. J Invest Dermatol.
2001 Oct;117(4):892-7. PMID: 11676829).
Sun block should be re-applied frequently depending on what you are
doing. A sign in the Dermatology Clinic at my hospital says "Wear
sun block all day, every day." A suntan is not enough to protect
you.
Besides causing the very common skin cancer, sunlight (along with
smoking) is responsible for much of the premature skin aging changes,
including wrinkles. If you wonder
if it really makes a difference, just look at the top and bottom of
your forearm. The top was exposed to the sun a lot: if you are like
me it is covered with spots, wrinkles, and blemishes. The bottom is
relatively protected and is child-like. The best protection is to
avoid exposure by wearing clothes and a hat; UV-protecting sunglasses
or polycarbonate glasses will protect your eyes and eyelids.
Potential
problems: Sunlight helps your body make the active form of vitamin D:
just make sure you get enough vitamin D in your diet.
Go
to TOC
Protein
When
I was growing up – indeed, until recently – I thought that the
primary sources of protein were meat, cheese, beans and nuts. Well…
there are two primary issues in choosing quality protein.
“Completeness”
of the protein: does the protein in your whole diet contain
enough of each of the essential amino acids? Protein from limited
vegetables alone may not be complete, while protein from meat is.
What
proportion of the food calories is from protein? For example, it
is easy to think that salmon is a better source of protein than
spinach. However, only 43% of the calories in salmon are protein,
while 50% of spinach’s calories are protein. Vegetables like
spinach and broccoli (43%) have more protein per calorie than
nuts (4-20%), peanut butter (19%), most meats, cheese (24%) or
skim milk (40%).
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Vegetable
protein
|
Lessens
risk of cholecystectomy (from gallstones)
|
From
the Nurses’ Health Study, “the relative risk for animal
protein intake was 1.07 (95% CI: 0.98, 1.15; p for trend = 0.08),
whereas the relative risk for vegetable protein intake was 0.79
(95% CI: 0.71, 0.88; p for trend < 0.0001), with a significant
dose-response relation… These results suggest that increased
consumption of vegetable protein in the context of an
energy-balanced diet can reduce the risk of cholecystectomy in
women.”
|
386
|
|
|
|
Good
for bone health (and animal protein is bad)
|
“Our
analysis includes 8,178 female study participants of the European
Prospective Investigation into Cancer and Nutrition (EPIC) Potsdam
Study. Ultrasound bone measurements were performed on the right os
calcis, and BUA was determined. Dietary intake was assessed by a
standardized food frequency questionnaire. We applied linear
regression models to estimate the association between dietary
protein and BUA. RESULTS: After multivariate adjustment, high
intake of animal protein was associated with decreased BUA values
(beta = -0.03; p = 0.010) whereas high vegetable protein intake
was related to an increased BUA (beta = 0.11; p = 0.007). The
effect of dietary animal protein on BUA was modified by calcium
intake. CONCLUSION: High consumption of protein from animal
origin may be unfavourable, whereas a higher vegetable protein
intake may be beneficial for bone health. Our results
strengthen the hypothesis that high calcium intake combined with
adequate protein intake based on a high ratio of vegetable to
animal protein may be protective against osteoporosis.”
|
387
|
|
|
Total
protein
|
Lessens
the risk of heart attack
|
“The
study was a prospective cohort study. RESULTS: We examined the
association between dietary protein intake and incidence of
ischemic heart disease in a cohort of 80082 women aged 34-59 y and
without a previous diagnosis of ischemic heart disease, stroke,
cancer, hypercholesterolemia, or diabetes in 1980. Intakes of
protein and other nutrients were assessed with validated dietary
questionnaires. We documented 939 major instances of ischemic
heart disease during 14 y of follow-up. After age, smoking, total
energy intake, percentages of energy from specific types of fat,
and other ischemic heart disease risk factors were controlled for,
high protein intakes were associated with a low risk of
ischemic heart disease; when extreme quintiles of total
protein intake were compared, the relative risk was 0.74 (95%
CI: 0.59, 0.94). Both animal and vegetable proteins contributed to
the lower risk. This inverse association was similar in women with
low- or high-fat diets.”
|
388
|
|
|
|
Lowers
BP and improves lipids
|
“Randomized,
3-period, crossover feeding study … Participants were 164 adults
with prehypertension or stage 1 hypertension. Each feeding period
lasted 6 weeks and body weight was kept constant. INTERVENTIONS: A
diet rich in carbohydrates; a diet rich in protein, about half
from plant sources; and a diet rich in unsaturated fat,
predominantly monounsaturated fat. MAIN OUTCOME MEASURES: Systolic
blood pressure and low-density lipoprotein cholesterol. RESULTS:
Blood pressure, low-density lipoprotein cholesterol, and estimated
coronary heart disease risk were lower on each diet compared with
baseline. Compared with the carbohydrate diet, the protein diet
further decreased mean systolic blood pressure by 1.4 mm Hg (P
= .002) and by 3.5 mm Hg (P = .006) among those with hypertension
and decreased low-density lipoprotein cholesterol by 3.3 mg/dL
(0.09 mmol/L; P = .01), high-density lipoprotein cholesterol by
1.3 mg/dL (0.03 mmol/L; P = .02), and triglycerides by 15.7 mg/dL
(0.18 mmol/L; P<.001). Compared with the carbohydrate diet, the
unsaturated fat diet decreased systolic blood pressure by 1.3
mm Hg (P = .005) and by 2.9 mm Hg among those with
hypertension (P = .02), had no significant effect on low-density
lipoprotein cholesterol, increased high-density lipoprotein
cholesterol by 1.1 mg/dL (0.03 mmol/L; P = .03), and lowered
triglycerides by 9.6 mg/dL (0.11 mmol/L; P = .02). Compared
with the carbohydrate diet, estimated 10-year coronary heart
disease risk was lower and similar on the protein and unsaturated
fat diets.”
|
291
|
|
Go
to TOC
Methionine
restriction
75%
reduction appears to slow the aging process and prolong lifespan in
rats. People can do something like this by eating vegetables instead
of meat: this results in a reduction of ~50% in methionine.
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Methionine
restriction
|
RESTRICTION
of this amino acid may slow aging and prolong life
…At
least in RATS
|
“A
diet deficient in the amino acid methionine has previously been
shown to extend lifespan in several stocks of inbred rats. We
report here that a methionine-deficient (Meth-R) diet also
increases maximal lifespan in … mice. Compared with controls,
Meth-R mice have significantly lower levels of serum IGF-I,
insulin, glucose and thyroid hormone. Meth-R mice also have higher
levels of liver mRNA for MIF (macrophage migration inhibition
factor), known to be higher in several other mouse models of
extended longevity. Meth-R mice are significantly slower to
develop lens turbidity and to show age-related changes in T-cell
subsets. They are also dramatically more resistant to oxidative
liver cell injury induced by injection of toxic doses of
acetaminophen. The spectrum of terminal illnesses in the Meth-R
group is similar to that seen in control mice. Studies of the
cellular and molecular biology of methionine-deprived mice may, in
parallel to studies of calorie-restricted mice, provide insights
into the way in which nutritional factors modulate longevity and
late-life illnesses.”
Note:
methionine is present in all natural proteins. Meats are highest
in methionine: typically 2.5 to 3.0% of meat and dairy protein is
methionine; typically 0.9 to 1.5% of vegetable protein is
methionine. Yet another reason to keep meat intake low, and eat
your veggies!
|
389
|
|
|
|
|
“… methionine
restriction-related life span extension is not a consequence of
reduced energy intake. By feeding the methionine restricted diet
to a variety of rat strains we determined that lowered methionine
in the diet prolonged life in strains that have differing
pathological profiles in aging, indicating that this intervention
acts by altering the rate of aging, not by correcting some single
defect in a single strain.”
|
390
|
|
|
|
|
“…lifelong
reduction in the concentration of a single dietary component, the
essential amino acid L-methionine, from 0.86 to 0.17% of the diet
results in a 30% longer life span of male Fischer 344
rats.”
|
391
|
|
|
|
Effects
are additive to CR
… in
rats
|
“Reduced
dietary methionine intake (0.17% methionine, MR) and calorie
restriction (CR) prolong lifespan in male Fischer 344 rats… MR
rats show significantly reduced visceral fat compared to CF and PF
with concomitant decreases in basal insulin, glucose, and leptin,
and increased adiponectin and triiodothyronine…In a separate
cohort, insulin responses of older MR animals as measured by oral
glucose challenge are similar to young animals. Longitudinal
assessments of MR and CF through 112 weeks of age reveal that MR
prevents age-associated increases in serum lipids… Collectively,
the results indicate that MR reduces visceral fat and preserves
insulin activity in aging rats independent of energy restriction.”
|
392
|
|
|
|
May
reduce risk of colon cancer
|
“[formation
of preneoplastic aberrant crypt foci (ACF)] formation was markedly
reduced in rats fed the MR diet with ACF containing >/= 4
crypts/focus being reduced by over 80% compared to controls...
These results show that MR inhibits colonic tumor development in
the rat, an effect that occurs primarily during post-initiation
phases of carcinogenesis and may be due, in part, to an inhibition
of colonic cell proliferation.”
|
393
|
|
|
|
May
NOT be additive to CR
|
“Recently,
methionine restriction has received wide acclaim including
speculation that it may play a role in FR-induced life extension.
In my opinion, work on rats done in our laboratory makes it
unlikely that this speculation is correct, at least for that
species (4). We found that a long term 40% reduction in food
intake without a reduction in methionine intake extends the life
of rats to the same extent as a 40% reduction of both food and
methionine intake does (Table 1). Thus, it is clear that
methionine intake need not be decreased for FR to markedly extend
the life of rats.”
|
394
|
|
Go
to TOC
Summaries
of preventative measures for specific diseases
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Alzheimer
Disease
|
|
Thorough
summary with lots of references, in a free PDF document.
“Epidemiology studies, including both regional incidence and the
analysis of specific risk factors for Alzheimer's disease indicate
that substantial prevention of the disease, in the 50-70 percent
range, is a practical possibility for the United States.”
|
395
|
|
|
Heart
disease
|
|
The
American Heart Association “Diet and Lifestyle Recommendations
Revision 2006” states: “Specific goals are to consume an
overall healthy diet; aim for a healthy body weight; aim for
recommended levels of low-density lipoprotein cholesterol,
high-density lipoprotein cholesterol, and triglycerides; aim for
normal blood pressure; aim for a normal blood glucose level; be
physically active; and avoid use of and exposure to tobacco
products. The recommendations are to balance caloric intake and
physical activity to achieve and maintain a healthy body weight;
consume a diet rich in vegetables and fruits; choose whole-grain,
high-fiber foods; consume fish, especially oily fish, at least
twice a week; limit intake of saturated fat to <7% of energy,
trans fat to <1% of energy, and cholesterol to <300 mg/day
by choosing lean meats and vegetable alternatives, fat-free (skim)
or low-fat (1% fat) dairy products and minimize intake of
partially hydrogenated fats; minimize intake of beverages and
foods with added sugars; choose and prepare foods with little or
no salt; if you consume alcohol, do so in moderation; and when you
eat food prepared outside of the home, follow these Diet and
Lifestyle Recommendations. By adhering to these diet and lifestyle
recommendations, Americans can substantially reduce their risk of
developing cardiovascular disease, which remains the leading cause
of morbidity and mortality in the United States.”
|
396
|
|
|
Osteoporosis
|
Avoid
colas
|
“Soft
drink consumption may have adverse effects on bone mineral density
(BMD), but studies have shown mixed results. In addition to
displacing healthier beverages, colas contain caffeine and
phosphoric acid (H(3)PO(4)), which may adversely affect bone.
OBJECTIVE: We hypothesized that consumption of cola is associated
with lower BMD. DESIGN: BMD was measured at the spine and 3 hip
sites in 1413 women and 1125 men in the Framingham Osteoporosis
Study by using dual-energy X-ray absorptiometry. Dietary intake
was assessed by food-frequency questionnaire. We regressed each
BMD measure on the frequency of soft drink consumption for men and
women after adjustment for body mass index, height, age, energy
intake, physical activity score, smoking, alcohol use, total
calcium intake, total vitamin D intake, caffeine from noncola
sources, season of measurement, and, for women, menopausal status
and estrogen use. RESULTS: Cola intake was associated with
significantly lower (P < 0.001-0.05) BMD at each hip site, but
not the spine, in women but not in men. The mean BMD of those with
daily cola intake was 3.7% lower at the femoral neck and 5.4%
lower at Ward's area than of those who consumed <1 serving
cola/mo. Similar results were seen for diet cola and, although
weaker, for decaffeinated cola. No significant relations between
noncola carbonated beverage consumption and BMD were observed.
Total phosphorus intake was not significantly higher in daily cola
consumers than in nonconsumers; however, the calcium-to-phosphorus
ratios were lower. CONCLUSIONS: Intake of cola, but not of other
carbonated soft drinks, is associated with low BMD in women.
Additional research is needed to confirm these findings.”
|
397
|
|
Go
to TOC
Brush
your teeth
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Brush
teeth
|
Periodontal
disease may => vascular disease
|
“multiple
logistic regression analysis identified periodontal
disease as a principal independent predictor of the
common carotid [disease]… The present results indicate that
periodontal disease is associated with the development
of early atherosclerotic carotid lesions.” So brush
your teeth!!
|
398
|
|
|
|
|
“Dental
status, oral hygiene, and particularly tooth loss are associated
with the degree of carotid stenosis and predict future progression
of the disease.”
|
399
|
|
|
|
Periodontal
disease may => prostate cancer
|
|
|
|
Go
to TOC
Safety
measures
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Hip
fracture prevention
|
Hip
protectors Reduce hip fractures by half
|
Hip
protectors reduce hip fractures by half in the elderly. “We
randomly assigned 1801 ambulatory but frail elderly adults (1409
women and 392 men; mean age, 82 years), … either to a group that
wore a hip protector or to a control group…The respective rates
of hip fracture were 21.3 and 46.0 per 1000 person-years.”
|
400
|
|
Go
to TOC
Genetics
|
Category
|
Effect
|
Finding
|
Ref
|
Fig
|
|
Lipoprotein
size
|
Lesser
small LDL and HDL particles was very strongly correlated
with human lifespan and overall health
|
“NMR-measured
lipoprotein profiles were analyzed in 165 families from the Leiden
Longevity Study, consisting of 340 long-lived siblings (females
>91 y, males >89 y), 511 of their offspring, and 243
partners of the offspring. Offspring had larger (21.3 versus 21.1
nm; p = 0.020) and fewer (1,470 versus 1,561 nmol/l; p = 0.011)
LDL particles than their same-aged partners. This effect was even
more prominent in the long-lived siblings (p < 10(-3)) and
could be pinpointed to a reduction specifically in the
concentration of small LDL particles. No differences were observed
for HDL particle phenotypes. The mean LDL particle sizes in 259
90-y-old singletons from a population-based study were similar to
those in the long-lived siblings and thus significantly larger
than in partners of the offspring, suggesting that the relevance
of this phenotype extends beyond familial longevity. A low
concentration of small LDL particles was associated with better
overall health among both long-lived siblings (p = 0.003) and
90-y-old singletons (p = 0.007). CONCLUSIONS: Our study indicates
that LDL particle profiles mark both familial and sporadic human
longevity already in middle age.”
|
401
|
|
Avoid
charring or browning meat: this
induces the formation of "heterocyclic amines"
(heterocyclic amines are carcinogens,
e.g. they cause cancer) and advanced
glycosylation end-products
(AGEs). Instead boil or low-power microwave it and reduce how
much you eat. This is probably most important for red meat (mammals
including beef and pork); the risk may be lower for white meat (fowl
& fish). A study from the University of South Carolina (reported
in Journal of the National Cancer Institute 1998-11-18) found a
five-fold increase in breast cancer rates in women who consistently
ate well-done red meat. Another study found a similarly increased
incidence of pancreatic cancer from food that was fried, smoked,
salty, high in refined sugar or dehydrated; and a low
incidence with raw food intake and the use of microwave ovens to
cook food (Cancer
Epidemiol Biomarkers Prev 1995 Dec;4(8):895-9; PMID: 8634663).
In addition, roasted nuts, cereal, milk products, etc. have AGEs;
probably it is best to eat these with as little cooking and at as
low temperatures as reasonable.
One study found that
“…dietary AGEs promote inflammatory mediators, leading to
tissue injury. Restriction of dietary AGEs suppresses these
effects.” (Vlassara
H, Cai W, Crandall J, Goldberg T, Oberstein R, Dardaine V, Peppa M,
Rayfield EJ. Inflammatory mediators are induced by dietary
glycotoxins, a major risk factor for diabetic angiopathy. Proc Natl
Acad Sci U S A. 2002 Nov 12. PMID: 12429856)
Processed
meats (such as hot dogs) also have been associated with an increased
risk of Type II diabetes (Diabetes
Care 2002 Mar;25(3):417-24; PMID: 11874924),
as well as an increased risk of colon cancer.
Contraindications:
None.
Potential problems: Meat does not taste quite as good.
Cooking
protein or fat in combination with simple sugars (glucose or
fructose, such as corn syrup, Bar-B-Q sauce, fruit, milk, etc. –
but NOT table sugar (sucrose)) will also cause formation of
substantial amounts of advanced
glycosylation end-products
(AGEs). 10% of these dietary AGEs are absorbed from the gut, and
only 30% of the absorbed AGEs are excreted by the kidneys. The rest
may be deposited around the body and cause an eventual toxic
buildup, as occurs in diabetics (Diabetes
Metab (Paris) 2001, 27, 535-542). The
known or hypothesized toxic effects of these AGEs are primarily
vascular. AGE
ingestion also is seems to raise the risk for diabetes in lab rats.
Note that AGEs are in nearly all food we eat – another
reason to be on caloric
restriction! This is especially
clearly seen in diabetics (“dietary restriction of AGE food
intake may greatly reduce the burden of AGEs in diabetic patients
and possibly improve prognosis.” Proc
Natl Acad Sci U S A 1997 Jun 10;94(12):6474-9; PMID: 9177242)
but in my opinion probably applies to all.
AGEs are tasty!
They are responsible for the good flavor of coffee (see Scientific
American, June 2002) and perhaps other foods such as grilled meat
and chocolate. While AGEs are in these foods it is not at all clear
that they are harmful. For example, coffee has been extensively
studied and has been found to be virtually harmless.
Whether
ingested AGEs are clinically significant for normal people is an open
question. Certainly AGEs formed in
the body – especially those associated with diabetes, smoking, and
sunlight exposure – are highly correlated with aging effects and
are inversely correlated with lifespan.
Contraindications:
None.
Potential problems: Meat does not taste quite as good.
Colon
cancer may be caused in part by red meat (doubles risk) and cured
meats (including bacon, cured ham, salami, corned beef and
pastrami). These meats cause the formation of carcinogenic N-nitroso
compounds by bacteria in the feces, and may thus be a risk factor in
colon cancer. Dairy products and soy do not (soy
may cause problems on estrogen-sensitive tissues and the thyroid,
but may also help prevent prostate cancer: whether it is beneficial
overall is unclear). It is probably best to avoid eating large
quantities of these meats. In addition, colon cancer risk may be
reduced by 40% by eating a high-fiber diet. Perhaps the major factor
associated with colon cancer is high body mass index. Factors that
may decrease the risk: legumes (beans), broccoli and the like,
NSAIDs, and folate. (Lipkin
M, Reddy B, Newmark H, Lamprecht SA. Dietary factors in human
colorectal cancer. Annu Rev Nutr. 1999;19:545-86. Review. PMID:
10448536)
Avoid
processed, cured and smoked meats such as hot dogs, bacon, smoked
foods and lunchmeats: nitrites and the smoke processing seem to be
the cause of much of stomach cancer. (Int
J Cancer 1999 Mar 15;80(6):852-6; PMID: 10074917: Of
various sources of N-nitroso compounds, intake of smoked and salted
fish was significantly (RR = 2.58, 95% CI 1.21-5.51) and intake of
cured meat was non-significantly (RR = 1.84, 95% CI 0.98-3.47)
associated with risk of colorectal cancer. No similar association
was observed for intake of other fish or other meat).
Smoked meats may be the cause of the very high stomach cancer rates
in Japan and Italy. Simultaneous vitamin C & E intake may
provide some protective effect against the carcinogenic properties
of nitrites, by helping prevent formation in the gut.
Contraindications: None.
Potential problems: None.
Many
of the foods that are best for your health are also full of oxalic
acid, a substance that causes kidney stones. No fun if you get them!
Fortunately, you can prevent the absorption of the oxalic acid in
your intestines by drinking milk (or taking some other source of
calcium: I prefer milk in fat-free cheese on my spinach: “Dietary
calcium lowers the risk of nephrolithiasis due to a decreased
absorption of dietary oxalate that is bound by intestinal calcium.”
Braz
J Med Biol Res 2002 Jun;35(6):669-75; PMID: 12045831,
and “Daily urine oxalate excretion/creatinine decreased
curvilinearly as estimated dietary Ca intake increased … as the
ratio of estimated dietary calcium to dietary oxalate increased”
Kidney
Int 1996 Jan;49(1):200-8; PMID: 8770968)
at the same meal you eat foods high in oxalate (spinach, rhubarb,
chard, beets, cocoa, peanuts, bran, berries, etc.) In addition, the
biggest risk factor for excretion of oxalate is body weight (Kidney
Int 1996 Jan;49(1):200-8; PMID: 8770968),
so if you are on CR this may not matter so much. For
a listing of oxalic acid levels in a variety of vegetables, check
this USDA web site or this
kidney stone prevention site. I
hypothesize that it is good to eat a milk-derived food when eating
the following: spinach, rhubarb, chard, okra, sweet potato, radish,
lettuce, carrots, green beans and Brussels sprouts (each of these –
especially the first three – has moderate concentrations of oxalic
acid and is often eaten in significant
amounts).
Contraindications: None.
Potential problems: None.
Eat
lots of vegetables and some fruit, especially tomatoes, broccoli
(broccoli
sprouts are best, and also other
vegetables in the cabbage family have the same protective effects),
purple grape juice, and berries (at least 1 cup and preferably 2
cups each day of blueberries, raspberries, and/or strawberries).
These seem to help prevent cancer and stroke.
The
American Institute for Cancer Research recommends five to 10
servings of fruits and vegetables a day for cancer protection.
Tomatoes (especially cooked) are the source of lycopene.
Lycopene
is available in highest concentrations in tomato paste, and may be
better absorbed if eaten with oil. “Among
72 studies identified, 57 reported inverse associations between
tomato intake or blood lycopene level and the risk of cancer at a
defined anatomic site; 35 of these inverse associations were
statistically significant… The evidence for a benefit was
strongest for cancers of the prostate, lung, and stomach.”
Giovannucci
E. Tomatoes, tomato-based products, lycopene, and cancer: review of
the epidemiologic literature. J Natl Cancer Inst. 1999 Feb
17;91(4):317-31. Review. PMID: 10050865.
Broccoli sprouts in particular have been found to have
especially high concentrations of glucoraphanins (10-50 times more
than mature flowerets), and have been shown to prevent and slow the
growth of breast cancer in rats (Proc
Natl Acad Sci U S A 1997 Sep 16;94(19):10367-72; PMID: 9294217).
To get sufficient protective quantities of glucoraphanins from
mature broccoli flowerets would require approximately 20% of your
food to be from broccoli alone. The benefits of eating
broccoli-family vegetables are probably due to induction by
glucoraphanins of “Phase 2 enzymes” that detoxify carcinogens,
rather than from any antioxidant effects.
Part of the
protection from eating lots of fruits and vegetables may simply be
avoidance of relatively bad food.
Contraindications:
None.
Potential problems: Gas. Try cooking the vegetables more or
eating different types and amounts.
Exercise
regularly and moderately (30 minutes each day). This has repeatedly
been shown to have several beneficial long-term health effects,
including substantially reduced rates of diabetes & (at least)
colon cancer, preservation of mental function & bone strength,
and reduced risk of cardiovascular disease (“Women in
increasing quintiles of energy expenditure measured in metabolic
equivalents (the MET score) had age-adjusted relative risks of
coronary events of 1.00, 0.73, 0.69, 0.68, and 0.47, respectively (P
for trend, <0.001). In multivariate analyses, the inverse
gradient between the total MET score and the risk of cardiovascular
events remained strong (adjusted relative risks for increasing
quintiles, 1.00, 0.89, 0.81, 0.78, and 0.72, respectively; P for
trend <0.001). Walking and vigorous exercise were associated with
similar risk reductions, and the results did not vary substantially
according to race, age, or body-mass index. A brisker walking pace
and fewer hours spent sitting daily also predicted lower risk.”
Lee
IM, Rexrode KM, Cook NR, Manson JE, Buring JE. Physical activity and
coronary heart disease in women: is "no pain, no gain"
passe? JAMA. 2001 Mar 21;285(11):1447-54. PMID: 11255420;
Manson
JE, Greenland P, LaCroix AZ, Stefanick ML, Mouton CP, Oberman A,
Perri MG, Sheps DS, Pettinger MB, Siscovick DS. Walking compared
with vigorous exercise for the prevention of cardiovascular events
in women. N Engl J Med. 2002 Sep 5;347(10):716-25. PMID: 12213942;
and from a 12-year study of 44,452 men: “Total physical activity,
running, weight training, and walking were each associated with
reduced CHD risk. Average exercise intensity was associated with
reduced risk…” Tanasescu
M, Leitzmann MF, Rimm EB, Willett WC, Stampfer MJ, Hu FB. Exercise
type and intensity in relation to coronary heart disease in men.
JAMA. 2002 Oct 23;288(16):1994-2000. PMID: 12387651).
There is also a suggestion that moderate exercise may be associated
with longer life, but the effect is hard to differentiate from other
lifestyle changes (Schnohr
P, Parner J, Lange P. [Joggers live longer. The Osterbro study]
Ugeskr Laeger. 2001 May 7;163(19):2633-5. Danish. PMID: 11360357;
Fraser
GE, Shavlik DJ. Ten years of life: Is it a matter of choice? Arch
Intern Med. 2001 Jul 9;161(13):1645-52. PMID: 11434797.)
Note
that over-exertion may be harmful, both directly on the joints, and
if you have to eat a lot to make up for calories used in exercise
this partially defeats caloric restriction principles. Exercise
helps keep your bones strong, helping to prevent
osteoporosis-related fractures.
Contraindications: Ask your
doctor first before starting an exercise program!
Potential
problems: The increased metabolism of exercise causes some free
radical induced damage and DNA damage. Exercise does NOT seem to
affect life span (Epidemiology
1997 Mar;8(2):168-74; PMID: 9229209)!
Instead, I think of it as a way to improve the life I have.
Floss
your teeth every day, in addition to brushing after every meal. This
reduces your risk for heart attack and stroke, probably by reducing
the chronic, low-grade gum infections.
Contraindications: None.
Potential problems: None.
Get
your vaccinations! Influenza and pneumonia kill lots of people,
especially after age 65 yr.
Most
supplements (except vitamins A, E, & B12) should be taken in
small doses several times each day instead of once a day. Just like
medications they are not stored in the body, lasting about 4 hours,
and thus may be best if taken three or four times per day. In my
opinion, this includes folate, red grapes (grape juice or grape seed
extract), tea, broccoli, and (for those with heart attack risk
factors) aspirin. An easy way to do this is to eat good food at
every meal and take supplements with each meal and at bedtime. You
should probably not take any supplemental vitamin A if you can avoid
it: too much is quite toxic, and most people get plenty in the
vegetables they eat.
Treat
any infections. Chronic sinusitis and gingivitis (bad oral health)
have been shown to predispose to heart disease!
Recently the
bacterium that causes stomach ulcers, Heliobacter pylori, has
been strongly associated with stomach cancer (N
Engl J Med 2001 Sep 13;345(11):784-9; PMID: 11556297).
They estimated that if this infection can be identified and treated
with antibiotics we could eliminate the #10 cause of cancer death in
America. Approximately 35% of Americans have H. pylori infection
and do not know it: this appears to be associated with a 2.9% risk
of this cancer. Fortunately, broccoli and broccoli sprouts contain a
beneficial nutrient (sulphorophane) that kills H. pylori, and
they contain it in sufficient concentrations to prevent this
infection.
If
you have risk factors for heart disease (obesity, high blood
pressure, diabetes, smoking, family history, etc.), consider taking
low-dose, non-buffered (the buffer has aluminum) aspirin, perhaps ¼
tablet every other day. This does two things:
Reduces
your risk for heart attacks (the #1 killer!) by 40%.
May
reduce your risk for colon cancer (the #2 cancer killer after lung
cancer - and you can avoid this by not smoking) by 20%.
May
reduce the overall risk for strokes (although it increases the risk
of a hemorrhagic stroke).
Do
not take both ibuprofen and aspirin together.
Contraindications:
stomach upset or gastritis with aspirin, bleeding problems. The
cardiac benefit may also not be worth the risks for those with few
risk factors for heard disease.
Potential problems: hemorrhagic
stroke, bleeding problems, stomach upset, gastrointestinal bleed (can
be very serious or deadly!), and if you have kidney problems it may
cause an increased rate of kidney failure. The risk/benefit ratio has
been worked out for cardiac problems: for this purpose it is best to
take aspirin only if you have cardiac risk factors. On the other
hand, I think that this analysis did not take the reduced colon
cancer risk into account.
Things
I think may be worth trying because they probably work or may work
The
risk of Alzheimer’s disease is lower in populations with higher
education, nonsteroidal anti-inflammatory drugs, wine consumption,
coffee consumption, and regular physical activity (Am
J Epidemiol 2002 Sep 1;156(5):445-53; PMID: 12196314).
Consider
taking some sort of non-steroidal anti-inflammatory drug (NSAID)
such as Motrin (SEE WARNING BELOW). This
probably reduces the risk for Alzheimer's disease and cataracts.
Low-dose aspirin appears not to do this. A recent study from Holland
of 7000 people (N
Engl J Med 2001 Nov 22;345(21):1515-21; PMID: 11794217)
showed an 80% drop in the incidence of Alzheimer’s for those
taking NSAIDs for more than 2 years. Low dose worked as well as high
dose. Another study showed that Motrin has a direct effect
preventing the production of the protein associated with
Alzheimer’s. The National Institute on Aging (NIA) launched a new
clinical trial at the end of January 2001, called the Alzheimer’s
Disease Anti-Inflammatory Prevention Trial (ADAPT), to test naproxen
and celecoxib (Celebrex) with regards to Alzheimer’s prevention.
So in 20 years we will know the answer – but that may be too late
for some of us! See Ophthalmology 2001;108:1400-1408. Also, the
combination of an NSAID and vitamin E reduces atherosclerosis in
mice with high cholesterol levels by 80% (Circulation
2001 Oct 16;104(16):1940-5; PMID: 11602498).
If you take ibuprofen (vs. Alzheimer’s disease, etc.) and aspirin
(vs. heart disease), be sure to take the aspirin first and wait for
about 2 hours: ibuprofen blocks the usefulness of aspirin.
Potential
problems: This is a potentially fatal drug. It can cause
bleeding problems, stomach upset, gastrointestinal bleed (can be very
serious!), liver and kidney problems. Be careful of long-term use!! –
I really am unsure on the long-term risk/benefit ratio of this one,
but since I have no stomach or renal problems, the several studies
indicating such a dramatic benefit had convinced me personally to
take low-dose Motrin two times each day. Unfortunately this also
caused me to become hyponatremic (low level of sodium found in a
blood test: no symptoms, but it could indicate potential for causing
kidney or other problems, so I stopped the Motrin.)
Glucosamine
and chondroitin may reduce the chance of getting osteoarthritis,
the most common kind of arthritis. Certainly they have been shown to
reduce the symptoms. Both of these are the body's natural joint
lubricants (JAMA
2000 Mar 15;283(11):1469-75; PMID: 10732937).
To get these you need to take tablets. “Dr.
Theo” has a comprehensive web
site discussion, with studies, analysis and recommendations. From
this site it appears that it is necessary for full effect to take
both glucosamine and chondroitin, and to take the chondroitin in
doses of at least 1200 mg/day. Because the chondroitin is expensive
and quite variable in the available formulations, the Dr. Theo site
recommends several brands shown to have high quality by HPLC
testing.
(Lancet
2001 Jan 27;357(9252):251-6; PMID: 11214126):
Two
hundred twelve patients with mild to moderate arthritis were
randomly assigned a 1500 mg daily glucosamine sulfate supplement or
a placebo for a period of three years in a double-blind trial.
X-ray films of the knee were taken at the beginning and the
conclusion of the study to measure joint space width, in order to
assess cartilage loss. The study participants completed
questionnaires in which symptoms such as pain, joint function and
stiffness were scored.
At the conclusion of the study,
participants who received the placebo had significant mean and
minimum joint-space narrowing, showing cartilage loss. The majority
of the group of 106 patients receiving glucosamine sulfate had no
significant joint-space narrowing. Evaluation of the questionnaires
showed an improvement of symptoms in the glucosamine group and a
worsening of symptoms in the placebo group. Even in the small group
of patients who received glucosamine and experienced joint-space
narrowing, symptomatic relief was noted.
Note:
Caloric Restriction has also been shown to significantly delay the
onset of osteoarthritis in dogs.
Potential problems: Get
good-quality supplements.
A
high-fiber diet probably helps prevent heart disease (J
Nutr 1999 Jul;129(7 Suppl):1457S-66S; PMID: 10395621).
This has been found to be strongly true from epidemiology (in
comparative studies of populations of people such as vegetarians and
7th-Day Adventists) and animal studies. This is true for
fiber from cereals (e.g., wheat & oat), fruits and vegetables.
“In general … soluble fibers, such as
psyllium, oat bran, guar and pectin, decrease serum
cholesterol and LDL cholesterol concentrations without
affecting serum triglycerides.” (Beans have
soluble fiber too.) “(Insoluble fibers such as) wheat bran
intake decreased serum triglyceride concentrations in
humans (but) does not have a significant effect on serum cholesterol
concentrations.” Part of this positive effect is
probably from associated nutrients. The reduction in cholesterol and
triglyceride is approximately 10%. For most people the most
important thing to reduce is cholesterol. In addition, high-fiber
diets tend to reduce overall food intake. Nonetheless, caloric
restriction itself has by far the greatest effect in reduction of
these risk factors. My take is to practice caloric restriction, and
include a balanced variety high-fiber, low-calorie foods as part of
this diet.
Both psyllium (Am
J Clin Nutr 2000 Feb;71(2):472-9; PMID: 10648260)
and guar
have been shown to decrease cholesterol levels significantly. If you
get these, start slowly!! Both increase the stool volume
substantially, resulting in several bowel movements each day. If you
eat too much you can get in real trouble from this, with abdominal
pain: follow the directions on the bottles. I like the finely-ground
psyllium-based Metamucil equivalent from Wal-Mart, mixed with a
little guar powder and ground cloves, then mixed with cold diet
orange soda. (weird, I know…)
If
you are a man, donate blood regularly (about three times per year)
and avoid iron supplements. Iron
is a pro-oxidant (as opposed to an anti-oxidant); it enhances the
production of the highly reactive and toxic hydroxyl radical, thus
stimulating oxidative damage. It is associated with chronic damage
to the brain, skin, liver, and muscle. Excess and even "normal"
iron levels can cause an increased risk for heart attacks. A recent
article (Ann
N Y Acad Sci 2002 Jun;967:342-51) showed
that patients with iron deficiency had much better heart disease
risk factors (lower BP, higher HDL, lower LDL, etc.); these probably
beneficial things were reversed by supplementing with iron! A major
review article in Diabetes stated that high iron levels seem to
cause diabetes type 2, and “Iron depletion has been
demonstrated to be beneficial in coronary artery responses,
endothelial dysfunction, insulin secretion, insulin action, and
metabolic control in type 2 diabetes” (Diabetes
2002 Aug;51(8):2348-54; PMID: 12145144; the
full text is at
http://www.medscape.com/viewarticle/439591_1);
another stated that iron may be “a major factor of
(accelerated) ageing.” (Polla
AS, Polla LL, Polla BS. Iron as the malignant spirit in successful
ageing. Ageing Res Rev. 2003 Jan;2(1):25-37. PMID: 12437994)
Potential problems: 1) Ouch! 2) You may develop iron-deficiency
anemia if you give too much blood. Not likely for most men: I had
been donating blood about four to six times per year and avoiding
iron supplements for about 25 yr., and only recently had low iron
levels – low enough to actually cause iron deficiency anemia
requiring supplements! Of note, it appears that both iron deficiency
and high-dose iron supplementation may cause mitochondrial damage
(Proc
Natl Acad Sci U S A 2002 Feb 19;99(4):2264-9; PMID: 11854522),
possibly the cause of most aging changes.
There
is one study that implies we should eat lots of protein: the higher
the protein, the longer the life span for both ad lib
(eat-what-you-want) and caloric restricted rodents. From this
post, about 75% down the message
(slightly edited):
-
|
Days
survived
|
Ad
lib
|
CR
|
|
protein
% =>
|
10
|
22
|
51
|
10
|
22
|
51
|
|
900
|
8
|
2
|
6
|
93
|
116
|
149
|
|
1000
|
0
|
0
|
1
|
48
|
85
|
122
|
|
1200
|
0
|
0
|
0
|
5
|
61
|
91
|
|
1300
|
0
|
0
|
0
|
0
|
31
|
59
|
|
1400
|
0
|
0
|
0
|
0
|
11
|
24
|
|
1500
|
0
|
0
|
0
|
0
|
1
|
10
|
|
1600
|
0
|
0
|
0
|
0
|
0
|
3
|
Further,
the highest-protein groups had the lowest ratios of malignant to
benign tumors, and the lowest AGE-SPECIFIC tumor rates of all
isocaloric groups: that is, the low-protein group had fewer cancers
only because they died sooner -- their rate of tumor formation was
higher. (Ross MH, Bras G.
Influence of protein under-and overnutrition on spontaneous tumor
prevalence in the rat. J Nutr 1973;103: 944-963.)
This
is only one study, and an old one at that, but they used a lot of
animals (1600) and I know of no contradictory evidence. However,
there are design and interpretation problems that limit the
usefulness of the study, such as their source of protein (casein),
carbohydrate (sugar) and fat (corn oil). It appears to me from
reading the paper that 1) older rats seemed to be the ones to most
benefit from a high protein diet, and 2) the CR rats needed the same
quantity of protein, but because their total diet was restricted they
did better on diets with a higher protein fraction.
Note:
older people may need proportionally more protein in their diet than
young people. A study of old rats showed that a 27% (by calories)
protein diet worked best for elderly rats, and noted in regard to
people that “Protein-energy malnutrition is common in the
elderly” (Walrand
S, Chambon-Savanovitch C, Felgines C, Chassagne J, Raul F, Normand B,
Farges MC, Beaufrere B, Vasson MP, Cynober L. Aging: a barrier to
renutrition? Nutritional and immunologic evidence in rats. Am J Clin
Nutr. 2000 Sep;72(3):816-24. PMID: 10966905).
Potential
problems: high-protein diets may cause 1) Problems for the kidneys,
that may not be a big problem for those on CR (Masoro
EJ, Iwasaki K, Gleiser CA, McMahan CA, Seo EJ, Yu BP. Dietary
modulation of the progression of nephropathy in aging rats: an
evaluation of the importance of protein. Am J Clin Nutr. 1989
Jun;49(6):1217-27. PMID: 2729159). 2)
Calcium loss and potential kidney stones (Reddy
ST, Wang CY, Sakhaee K, Brinkley L, Pak CY. Effect of
low-carbohydrate high-protein diets on acid-base balance,
stone-forming propensity, and calcium metabolism. Am J Kidney Dis.
2002 Aug;40(2):265-74. PMID: 12148098).
Reducing
salt intake may decrease your risk of high blood pressure, which in
turn affects heart disease and stroke. A study of actual salt intake
(measured by urinary sodium excretion) as a risk factor, high sodium
intake predicted mortality and risk of coronary heart disease,
independent of other cardiovascular risk factors, including blood
pressure. The hazards ratios for coronary heart disease,
cardiovascular disease, and all-cause mortality, associated with a
100 mmol increase in 24 h urinary sodium excretion, were 1.51 (95%
CI 1.14-2.00), 1.45 (1.14-1.84), and 1.26 (1.06-1.50), respectively,
in both men and women. (Tuomilehto
J, Jousilahti P, Rastenyte D, Moltchanov V, Tanskanen A, Pietinen P,
Nissinen A. Urinary sodium excretion and cardiovascular mortality in
Finland: a prospective study. Lancet. 2001 Mar 17;357(9259):848-51.
PMID: 11265954.)
However, there was a significant interaction between sodium
excretion and body mass index for cardiovascular and total
mortality; sodium predicted mortality in men who were overweight.
Thus much or most of the correlation may be due to weight alone.
Certainly short-term salt intake modulates blood pressure; the
long-term effects in thin people are not clear to me. I still like
my foods to taste good!
Another study states that the long-term
effects of a low-salt diet seem to be uncertain. “Without
knowledge of the sum of the multiple effects of a reduced sodium
diet, no single universal prescription for sodium intake can be
scientifically justified.” (Grassi
G, Dell'Oro R, Seravalle G, Foglia G, Trevano FQ, Mancia G. Short-
and long-term neuroadrenergic effects of moderate dietary sodium
restriction in essential hypertension. Circulation. 2002 Oct
8;106(15):1957-61. PMID: 12370219)
Aluminum
may cause Alzheimer's disease.
The evidence on this is unclear: there is some epidemiologic data to
support it, and aluminum is found in Alzheimer’s brain plaques.
Studies are hard to do, of course! Aluminum-based antiperspirants
may be the worst cause, perhaps because of absorption rates. On the
other hand, aluminum-based antacids (Mylanta etc.) may be safe.
Aluminum is also found in baking powder (sodium aluminum sulfate),
buffered aspirin and some pickles (alum).
Vitamin
E may reduce the risk of prostate cancer, perhaps by 1/3, and may
reduce the incidence of carotid vascular disease (Am
J Clin Nutr 2002 Sep;76(3):582-7; PMID: 12198003).
There are two main forms available: alpha tocophererol (from
almonds, hazelnuts, olive oil and avocado; this is the standard
vitamin E supplement) and gamma tocophererol (best source is peas;
also in pecans & walnuts, and to a lesser extent from cashews)
Peanuts do not have any vitamin E. Generally if supplements are
taken (as opposed to natural sources such as nuts), the alpha form
should be taken only with the gamma as well: both are needed, and
too much alpha actually leads to depletion of gamma (Am
J Clin Nutr 2001 Dec;74(6):714-22; PMID: 11722951).
Indeed, supplementation with vitamin E has been shown to be harmful
to the elderly in fighting off respiratory infections (JAMA
2002 Aug 14;288(6):715-21; PMID: 12169075);
Other studies show it is NOT beneficial to the heart, and may cause
other harm. I think it is better to eat a variety of nuts, which in
addition have monounsaturated fats and have been shown in
epidemiologic studies to be good for you.
Besides
the tocophererols, tocotrienols are a variant of vitamin E and are
found in palm oil and some grains. It may be best to get all of
these forms of vitamin E. Again,
I think that good foods are the best source, not high-dose
supplements.
Selenium
may possibly reduce overall cancer rates by up to 50% (based
indirectly on just one study that needs confirmation). Selenium is a
necessary part of the body’s anti-oxidant system. Glutathione
peroxidase is a selenium-dependant enzyme found primarily in the
cytoplasm (70%) but also in the mitochondria (30%). Requiring four
selenium atoms per active molecule, this enzyme scavenges lipid
peroxides throughout the membrane surfaces and quenches H2O2,
converting it to water. Evidence exists that supplementation with
selenium is able to increase the levels of glutathione peroxidase in
patients. Selenium is found in nuts (especially Brazil nuts, though
in quite variable concentrations; (Brazil nuts may be prone to toxic
fungus growth402
(aspergillus); they also have a lot of omega 6 and saturated fats: I
avoid them)) and supplements.
Caveat: too much can be toxic,
causing hair loss and skin problems.
Grazing
vs. two or three square meals. How you eat your meals may make a
difference. Here is one instance where common wisdom is probably
wrong: it is probably best to have very small meals with snacks in
between – as long as the total calorie intake is the same – and
restricted – of course! One study showed the grazing habit was
associated with lower cholesterol & vascular disease (J
Cardiovasc Risk 1999 Feb;6(1):19-22; PMID: 10197288).
This is just one study, but it seems to have been well-done, with
very significant results (P < 0.001 for both measurements), and
makes sense in light of other data. The reasons might be as follows:
small meals lead to lesser increases in levels of post-prandial
glucose, fats, insulin, etc., with resulting lesser damage from
these things.
Problem: needs confirmation.
Incidentally,
studies also show that it is easier for people to eat fewer calories
if the food is relatively bulky (i.e., not rich). This is a
behavioral aide, but also corresponds with eating more nutritional
foods such as vegetables.
References
3
Modified from Gruber RP, Kalamas AD. Measuring human
age by estimating lifetime caloric consumption. Gerontology 2000
Jan-Feb;46(1):44-6; PMID:
11111228
4
Field AE, Coakley EH, Must A, Spadano JL, Laird N, Dietz WH, Rimm
E, Colditz GA. Impact of overweight on the risk of developing
common chronic diseases during a 10-year period. Arch Intern Med.
2001 Jul 9;161(13):1581-6. PMID:
11434789
5
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R;
Prospective Studies Collaboration. Age-specific relevance of
usual blood pressure to vascular mortality: a meta-analysis of
individual data for one million adults in 61 prospective studies.
Lancet. 2002 Dec 14;360(9349):1903-13. PMID:
12493255
6
Nissen SE, Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA,
Crowe T, Howard G, Cooper CJ, Brodie B, Grines CL, DeMaria AN;
REVERSAL Investigators. Effect of intensive compared with
moderate lipid-lowering therapy on progression of coronary
atherosclerosis: a randomized controlled trial. JAMA. 2004 Mar
3;291(9):1071-80. PMID:
14996776
7
Atzmon G, Gabriely I, Greiner W, Davidson D, Schechter C,
Barzilai N. Plasma HDL levels highly correlate with cognitive
function in exceptional longevity. J Gerontol A Biol Sci Med Sci.
2002 Nov;57(11):M712-5. PMID:
12403798
8
Jorgensen L, Jenssen T, Joakimsen O, Heuch I, Ingebretsen OC,
Jacobsen BK. Glycated Hemoglobin Level Is Strongly Related to
the Prevalence of Carotid Artery Plaques With High Echogenicity in
Nondiabetic Individuals. The Tromso Study. Circulation. 2004 Jul 12
[Epub ahead of print] PMID:
15249512
9
Normal fasting plasma glucose levels and type 2 diabetes in young
men. N Engl J Med. 2005 Oct 6;353(14):1454-62. PMID:
16207847
11
de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle
N. Mediterranean diet, traditional risk factors, and the rate of
cardiovascular complications after myocardial infarction: final
report of the Lyon Diet Heart Study. Circulation. 1999 Feb
16;99(6):779-85. PMID:
9989963
Free
full text at http://circ.ahajournals.org/cgi/content/full/99/6/779
12
Daviglus ML, Stamler J, Pirzada A, Yan LL, Garside DB, Liu K,
Wang R, Dyer AR, Lloyd-Jones DM, Greenland P. Favorable
cardiovascular risk profile in young women and long-term risk of
cardiovascular and all-cause mortality. JAMA. 2004 Oct
6;292(13):1588-92. PMID:
15467061
13
Jolly CA, Muthukumar A, Avula CP, Troyer D, Fernandes G. Life
span is prolonged in food-restricted autoimmune-prone (NZB x
NZW)F(1) mice fed a diet enriched with (n-3) fatty acids. J Nutr.
2001 Oct;131(10):2753-60. PMID:
11584100; Full
text
14
Ross MH, Bras G. Influence of protein under- and
overnutrition on spontaneous tumor prevalence in the rat. J Nutr.
1973 Jul;103(7):944-63. No abstract available. PMID: 4351915
16
Liu J, Atamna H, Kuratsune H, Ames BN. Delaying brain
mitochondrial decay and aging with mitochondrial antioxidants and
metabolites. Ann N Y Acad Sci. 2002 Apr;959:133-66. Review. PMID:
11976193
17
Sharman EH, Vaziri ND, Ni Z, Sharman KG, Bondy SC. Reversal
of biochemical and behavioral parameters of brain aging by melatonin
and acetyl L-carnitine. Brain Res. 2002 Dec 13;957(2):223-30. PMID:
12445964
20
Siener R, Hesse A. The effect of a vegetarian and different
omnivorous diets on urinary risk factors for uric acid stone
formation. Eur J Nutr. 2003 Dec; 42(6): 332-7. PMID:
14673606
21
Key TJ, Fraser GE, Thorogood M, Appleby PN, Beral V, Reeves G,
Burr ML, Chang-Claude J, Frentzel-Beyme R, Kuzma JW, Mann J,
McPherson K. Mortality in vegetarians and nonvegetarians:
detailed findings from a collaborative analysis of 5 prospective
studies. Am J Clin Nutr. 1999 Sep;70(3 Suppl):516S-524S. PMID:
10479225 free
full text
22
Singh PN, Sabate J, Fraser GE. Does low meat consumption
increase life expectancy in humans? Am J Clin Nutr. 2003 Sep;78(3
Suppl):526S-532S. Review. PMID:
12936945
23
Choi HK, Atkinson K, Karlson EW, Willett W, Curhan G. Purine-rich
foods, dairy and protein intake, and the risk of gout in men. N Engl
J Med. 2004 Mar 11;350(11):1093-103. PMID:
15014182
24
Fung TT, Schulze M, Manson JE, Willett WC, Hu FB. Dietary
Patterns, Meat Intake, and the Risk of Type 2 Diabetes in Women.
Arch Intern Med. 2004 Nov 8;164(20):2235-2240. PMID:
15534160
26
Le Marchand L, Donlon T, Seifried A, Wilkens LR. Red meat
intake, CYP2E1 genetic polymorphisms, and colorectal cancer risk.
Cancer Epidemiol Biomarkers Prev. 2002 Oct;11(10 Pt 1):1019-24.
PMID:
12376502
27
Butler LM, Sinha R, Millikan RC, Martin CF, Newman B, Gammon MD,
Ammerman AS, Sandler RS. Heterocyclic amines, meat intake, and
association with colon cancer in a population-based study. Am J
Epidemiol. 2003 Mar 1;157(5):434-45. PMID:
12615608
28
Sandhu MS, White IR, McPherson K. Systematic review of the
prospective cohort studies on meat consumption and colorectal cancer
risk: a meta-analytical approach. Cancer Epidemiol Biomarkers Prev.
2001 May;10(5):439-46. PMID: 11352852 free
full text
29
Jiang R, Ma J, Ascherio A, Stampfer MJ, Willett WC, Hu FB.
Dietary iron intake and blood donations in relation to risk of
type 2 diabetes in men: a prospective cohort study. Am J Clin Nutr.
2004 Jan;79(1):70-5. PMID:
14684399
32
Meat intake and bladder cancer risk in 2 prospective cohort studies.
Am J Clin Nutr. 2006 Nov;84(5):1177-83. PMID:
17093172
33
Boltri JM, Akerson MR, Vogel RL. Aspirin prophylaxis in
patients at low risk for cardiovascular disease: a systematic review
of all-cause mortality. J Fam Pract. 2002 Aug;51(8):700-4. Review.
PMID:
12184966
34
Hayden M, Pignone M, Phillips C, Mulrow C. Aspirin for the
primary prevention of cardiovascular events: a summary of the
evidence for the U.S. Preventive Services Task Force. Ann Intern
Med. 2002 Jan 15;136(2):161-72. PMID:
11790072
35
Bosetti C, Talamini R, Franceschi S, Negri E, Garavello W,
Vecchia CL. Aspirin use and cancers of the upper aerodigestive
tract. Br J Cancer. 2003 Mar 10;88(5):672-4. PMID:
12618872
36
Baron JA, Cole BF, Sandler RS, Haile RW, Ahnen D, Bresalier R,
McKeown-Eyssen G, Summers RW, Rothstein R, Burke CA, Snover DC,
Church TR, Allen JI, Beach M, Beck GJ, Bond JH, Byers T, Greenberg
ER, Mandel JS, Marcon N, Mott LA, Pearson L, Saibil F, van Stolk RU.
A randomized trial of aspirin to prevent colorectal adenomas. N
Engl J Med. 2003 Mar 6;348(10):891-9. PMID:
12621133
37
Suji G, Sivakami S. Glucose, glycation and aging.
Biogerontology. 2004;5(6):365-73. PMID:
15609100
38
Lingelbach LB, Mitchell AE, Rucker RB, McDonald RB. Accumulation
of advanced glycation endproducts in aging male Fischer 344 rats
during long-term feeding of various dietary carbohydrates. J Nutr.
2000 May;130(5):1247-55. PMID:
10801926 free full text at
39
Hofmann SM, Dong HJ, Li Z, Cai W, Altomonte J, Thung SN, Zeng F,
Fisher EA, Vlassara H. Improved insulin sensitivity is
associated with restricted intake of dietary glycoxidation products
in the db/db mouse. Diabetes. 2002 Jul;51(7):2082-9. PMID:
12086936
41Goldberg
T, Cai W, Peppa M, Dardaine V, Baliga BS, Uribarri J, Vlassara H.
Advanced glycoxidation end products in commonly consumed foods. J Am
Diet Assoc. 2004 Aug;104(8):1287-91. PMID:
15281050
42
Adverse effects of dietary glycotoxins on wound healing in
genetically diabetic mice. Diabetes. 2003 Nov;52(11):2805-13. PMID:
14578300
45
Prevention of diabetic nephropathy in mice by a diet low in
glycoxidation products. Diabetes Metab Res Rev. 2002
May-Jun;18(3):224-37. Erratum in: Diabetes Metab Res Rev. 2002
Jul-Aug;18(4):332. PMID:
12112941
46
Jorgensen L, Jenssen T, Joakimsen O, Heuch I, Ingebretsen OC,
Jacobsen BK. Glycated Hemoglobin Level Is Strongly Related to
the Prevalence of Carotid Artery Plaques With High Echogenicity in
Nondiabetic Individuals. The Tromso Study. Circulation. 2004 Jul 12
[Epub ahead of print] PMID:
15249512
47
Gerstein HC. Glycosylated hemoglobin: finally ready for prime
time as a cardiovascular risk factor. Ann Intern Med. 2004 Sep
21;141(6):475-6. No abstract available. PMID: 15381522
48
Khaw KT, Wareham N, Bingham S, Luben R, Welch A, Day N.
Association of hemoglobin A1c with cardiovascular disease and
mortality in adults: the European prospective investigation into
cancer in Norfolk. Ann Intern Med. 2004 Sep 21;141(6):413-20. PMID:
15381514
49
The predictive role of blood glucose for mortality in subjects with
cardiovascular disease. Am J Epidemiol. 2006 Feb 15;163(4):342-51.
Epub 2005 Dec 22. PMID:
16373527
50
Metz TO, Alderson NL, Thorpe SR, Baynes JW. Pyridoxamine, an
inhibitor of advanced glycation and lipoxidation reactions: a novel
therapy for treatment of diabetic complications. Arch Biochem
Biophys. 2003 Nov 1;419(1):41-9. Review. PMID:
14568007
51
Hammes HP, Du X, Edelstein D, Taguchi T, Matsumura T, Ju Q, Lin
J, Bierhaus A, Nawroth P, Hannak D, Neumaier M, Bergfeld R, Giardino
I, Brownlee M. Benfotiamine blocks three major pathways of
hyperglycemic damage and prevents experimental diabetic retinopathy.
Nat Med. 2003 Mar;9(3):294-9. PMID:
12592403
52
Midaoui AE, Elimadi A, Wu L, Haddad PS, de Champlain J. Lipoic
acid prevents hypertension, hyperglycemia, and the increase in heart
mitochondrial superoxide production. Am J Hypertens. 2003
Mar;16(3):173-9. PMID:
12620694
53
Jorgensen L, Jenssen T, Joakimsen O, Heuch I, Ingebretsen OC,
Jacobsen BK. Glycated hemoglobin level is strongly related to
the prevalence of carotid artery plaques with high echogenicity in
nondiabetic individuals: the Tromso study. Circulation. 2004 Jul
27;110(4):466-70. Epub 2004 Jul 12. PMID:
15249512
54
Borugian MJ, Sheps SB, Whittemore AS, Wu AH, Potter JD, Gallagher
RP. Carbohydrates and colorectal cancer risk among Chinese in
North America. Cancer Epidemiol Biomarkers Prev. 2002
Feb;11(2):187-93. PMID:
11867506
55
Facchini FS, Saylor KL. A Low-Iron-Available,
Polyphenol-Enriched, Carbohydrate-Restricted Diet to Slow
Progression of Diabetic Nephropathy. Diabetes. 2003
May;52(5):1204-1209. PMID:
12716753
56
Ceriello A, Hanefeld M, Leiter L, Monnier L, Moses A, Owens D,
Tajima N, Tuomilehto J. Postprandial glucose regulation and
diabetic complications. Arch Intern Med. 2004 Oct 25;164(19):2090-5.
PMID:
15505121
57
Brownlee M. Biochemistry and molecular cell biology of
diabetic complications. Nature. 2001 Dec 13;414(6865):813-20. PMID:
11742414
58
Normal fasting plasma glucose levels and type 2 diabetes in young
men. N Engl J Med. 2005 Oct 6;353(14):1454-62. PMID:
16207847
61
Schulze MB, Liu S, Rimm EB, Manson JE, Willett WC, Hu FB.
Glycemic index, glycemic load, and dietary fiber intake and
incidence of type 2 diabetes in younger and middle-aged women. Am J
Clin Nutr. 2004 Aug;80(2):348-56. PMID:
15277155
62
Augustin LS, Galeone C, Dal Maso L, Pelucchi C, Ramazzotti V,
Jenkins DJ, Montella M, Talamini R, Negri E, Franceschi S, La
Vecchia C. Glycemic index, glycemic load and risk of prostate
cancer. Int J Cancer. 2004 Nov 10;112(3):446. PMID:
15382070
63
Slyper A, Jurva J, Pleuss J, Hoffmann R, Gutterman D. Influence
of glycemic load on HDL cholesterol in youth. Am J Clin Nutr. 2005
Feb;81(2):376-9. PMID:
15699224
64
Oh K, Hu FB, Cho E, Rexrode KM, Stampfer MJ, Manson JE, Liu S,
Willett WC. Carbohydrate intake, glycemic index, glycemic load,
and dietary fiber in relation to risk of stroke in women. Am J
Epidemiol. 2005 Jan 15;161(2):161-9. PMID:
15632266
65
The lifetime risk of stroke: estimates from the framingham study.
Stroke. 2006 Feb;37(2):345-50. Epub 2006 Jan 5. PMID:
16397184
66
Dietary carbohydrate intake and glycemic index in relation to
cortical and nuclear lens opacities in the Age-Related Eye Disease
Study. Am J Clin Nutr. 2006 May;83(5):1177-84. PMID:
16685063
67
Carbohydrate intake and glycemic index in relation to the odds of
early cortical and nuclear lens opacities. Am J Clin Nutr. 2005
Jun;81(6):1411-6. PMID:
15941895
68
Brand-Miller JC, Thomas M, Swan V, Ahmad ZI, Petocz P, Colagiuri
S. Physiological validation of the concept of glycemic load in
lean young adults. J Nutr. 2003 Sep;133(9):2728-32. PMID:
12949357
69
Wu LY, Juan CC, Hwang LS, Hsu YP, Ho PH, Ho LT. Green tea
supplementation ameliorates insulin resistance and increases glucose
transporter IV content in a fructose-fed rat model. Eur J Nutr. 2004
Apr;43(2):116-24. Epub 2004 Jan 06. PMID: 15083319
71
Archer VE. Does dietary sugar and fat influence longevity?
Med Hypotheses. 2003 Jun;60(6):924-9. PMID:
12699727
72
Consumption of sugar and sugar-sweetened foods and the risk of
pancreatic cancer in a prospective study. Am J Clin Nutr. 2006
Nov;84(5):1171-6. PMID:
17093171
73
Kris-Etherton
PM, Harris WS, Appel LJ. Omega-3 fatty acids and
cardiovascular disease: new recommendations from the American Heart
Association. Arterioscler Thromb Vasc Biol. 2003 Feb 1;23(2):151-2.
Review. PMID: 12588750
74
Kris-Etherton P, Daniels SR, Eckel RH, Engler M, Howard BV,
Krauss RM, Lichtenstein AH, Sacks F, St Jeor S, Stampfer M, Grundy
SM, Appel LJ, Byers T, Campos H, Cooney G, Denke MA, Kennedy E,
Marckmann P, Pearson TA, Riccardi G, Rudel LL, Rudrum M, Stein DT,
Tracy RP, Ursin V, Vogel RA, Zock PL, Bazzarre TL, Clark J. AHA
scientific statement: summary of the Scientific Conference on
Dietary Fatty Acids and Cardiovascular Health. Conference summary
from the Nutrition Committee of the American Heart Association. J
Nutr. 2001 Apr;131(4):1322-6. No abstract available. PMID: 11285345
Free
full text
75
Siscovick DS, Lemaitre RN, Mozaffarian D. The fish story: a
diet-heart hypothesis with clinical implications: n-3
polyunsaturated fatty acids, myocardial vulnerability, and sudden
death. Circulation. 2003 Jun 3;107(21):2632-4. PMID:
12782612
76
Tiemeier H, Van Tuijl HR, Hofman A, Kiliaan AJ, Breteler MM.
Plasma fatty acid composition and depression are associated in
the elderly: the Rotterdam Study. Am J Clin Nutr. 2003
Jul;78(1):40-46. PMID:
12816769
77
Erkkila AT, Lehto S, Pyorala K, Uusitupa MI. n-3 Fatty acids
and 5-y risks of death and cardiovascular disease events in patients
with coronary artery disease. Am J Clin Nutr. 2003 Jul;78(1):65-71.
PMID:
12816772
78
Bouwstra H, Dijck-Brouwer DJ, Wildeman JA, Tjoonk HM, Van Der
Heide JC, Boersma ER, Muskiet FA, Hadders-Algra M. Long-chain
polyunsaturated fatty acids have a positive effect on the quality of
general movements of healthy term infants. Am J Clin Nutr. 2003
Aug;78(2):313-318. PMID:
12885715
79
Helland IB, Smith L, Saarem K, Saugstad OD, Drevon CA. Maternal
supplementation with very-long-chain n-3 fatty acids during
pregnancy and lactation augments children's IQ at 4 years of age.
Pediatrics. 2003 Jan;111(1):e39-44. PMID:
12509593
80
Gago-Dominguez M, Yuan JM, Sun CL, Lee HP, Yu MC. Opposing
effects of dietary n-3 and n-6 fatty acids on mammary
carcinogenesis: The Singapore Chinese Health Study. Br J Cancer.
2003 Nov 3;89(9):1686-92. PMID:
14583770
81
Mamalakis G, Tornaritis M, Kafatos A. Depression and adipose
essential polyunsaturated fatty acids. Prostaglandins Leukot Essent
Fatty Acids. 2002 Nov;67(5):311-8. PMID:
12445491
82
Rajaram S, Burke K, Connell B, Myint T, Sabate J. A
monounsaturated fatty acid-rich pecan-enriched diet favorably alters
the serum lipid profile of healthy men and women. J Nutr. 2001
Sep;131(9):2275-9. PMID:
11533266
83
Sabate J. Nut consumption, vegetarian diets, ischemic heart
disease risk, and all-cause mortality: evidence from epidemiologic
studies. Am J Clin Nutr. 1999 Sep;70(3 Suppl):500S-503S. Review.
PMID: 10479222 free
full text
86
Tsai CJ, Leitzmann MF, Hu FB, Willett WC, Giovannucci EL. A
Prospective Cohort Study of Nut Consumption and the Risk of
Gallstone Disease in Men. Am J Epidemiol. 2004 Nov
15;160(10):961-968. PMID:
15522852
87
Mukuddem-Petersen J, Oosthuizen W,
Jerling JC. A Systematic Review of the Effects of Nuts
on Blood Lipid Profiles in Humans. J. Nutr. 135:2082-2089, September
2005. REF
88
Nuts, body weight and insulin resistance. Br J Nutr. 2006 Nov;96
Suppl 2:S79-86. PMID:
17125537
89
Morgan JM, Horton K, Reese D, Carey C, Walker K, Capuzzi DM.
Effects of walnut consumption as part of a low-fat,
low-cholesterol diet on serum cardiovascular risk factors. Int J
Vitam Nutr Res. 2002 Oct;72(5):341-7. PMID:
12463111
90
Ros E, Nunez I, Perez-Heras A, Serra M, Gilabert R, Casals E,
Deulofeu R. A Walnut Diet Improves Endothelial Function in
Hypercholesterolemic Subjects. A Randomized Crossover Trial.
Circulation. 2004 Mar 22 [Epub ahead of print] PMID:
15037535
91
Joan Sabaté, Ella Haddad, Jay S
Tanzman, Pera Jambazian and Sujatha Rajaram. Serum
lipid response to the graduated enrichment of a Step I diet with
almonds: a randomized feeding trial. Am J Clin Nutr. 2003
Jun;77(6):1379-84. PMID:
12791613
92
Wien MA, Sabate JM, Ikle DN, Cole SE, Kandeel FR. Almonds vs
complex carbohydrates in a weight reduction program. Int J Obes
Relat Metab Disord. 2003 Nov;27(11):1365-72. PMID:
14574348
93
Garg ML, Blake RJ, Wills RB. Macadamia Nut Consumption Lowers
Plasma Total and LDL Cholesterol Levels in Hypercholesterolemic Men.
J Nutr. 2003 Apr;133(4):1060-3. PMID:
12672919
94
Kritchevsky D, Tepper SA, Klurfeld DM. Lectin may contribute
to the atherogenicity of peanut oil. Lipids. 1998 Aug;33(8):821-3.
PMID:
9727614
95
Satchithanandam S, Flynn TJ, Calvert RJ, Kritchevsky D. Effect
of peanut oil and randomized peanut oil on cholesterol and oleic
acid absorption, transport, and distribution in the lymph of the
rat. Lipids. 1999 Dec;34(12):1305-11. PMID:
10652990
97
Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary
fatty acids and carbohydrates on the ratio of serum total to HDL
cholesterol and on serum lipids and apolipoproteins: a meta-analysis
of 60 controlled trials. Am J Clin Nutr. 2003 May;77(5):1146-55.
PMID:
12716665
99
Dietary Saturated Fat Intake Is Inversely Associated with Bone
Density in Humans: Analysis of NHANES III. J Nutr. 2006
Jan;136(1):159-65. PMID:
16365076
101
Dietary fat and serum lipids: an evaluation of the experimental
data. Am J Clin Nutr. 1993 Jun;57(6):875-83. Review. Erratum in: Am
J Clin Nutr 1993 Aug;58(2):245. PMID:
8503356
102
Morris MC, Evans DA, Bienias JL, Tangney CC, Bennett DA, Aggarwal
N, Schneider J, Wilson RS. Dietary fats and the risk of incident
Alzheimer disease. Arch Neurol. 2003 Feb;60(2):194-200. PMID:
12580703
103
Dietary fat intake and the risk of coronary heart disease in women.
N Engl J Med. 1997 Nov 20;337(21):1491-9. PMID:
9366580
104
Logroscino G, Marder K, Cote L, Tang MX, Shea S, Mayeux R.
Dietary lipids and antioxidants in Parkinson's disease: a
population-based, case-control study. Ann Neurol. 1996
Jan;39(1):89-94. PMID:
8572672
105
Robertson MD, Jackson KG, Fielding BA, Williams CM, Frayn KN.
Acute effects of meal fatty acid composition on insulin
sensitivity in healthy post-menopausal women. Br J Nutr. 2002
Dec;88(6):635-40. PMID:
12493085
106
Stender S, Dyerberg J. Influence of Trans Fatty Acids on
Health. Ann Nutr Metab. 2004 [Epub ahead of print] PMID:
14679314
107
Bolte G, Winkler G, Holscher B, Thefeld W, Weiland SK, Heinrich
J. Margarine Consumption, Asthma, and Allergy in Young Adults:
Results of the German National Health Survey 1998. Ann Epidemiol.
2005 Mar;15(3):207-213. PMID:
15723766
108
Sanders TA. High- versus low-fat diets in human diseases.
Curr Opin Clin Nutr Metab Care. 2003 Mar;6(2):151-5. PMID:
12589184
109
Calder PC, Deckelbaum RJ. Fat as a physiological regulator:
the news gets better. Curr Opin Clin Nutr Metab Care. 2003
Mar;6(2):127-31. PMID:
12589182
110
Strychar I, Ishac A, Rivard M, Lussier-Cacan S, Beauregard H,
Aris-Jilwan N, Radwan F, Yale JF. Impact of a
high-monounsaturated-fat diet on lipid profile in subjects with type
1 diabetes. J Am Diet Assoc. 2003 Apr;103(4):467-474. PMID:
12669010
111
Gill JM, Brown JC, Caslake MJ, Wright DM, Cooney J, Bedford D,
Hughes DA, Stanley JC, Packard CJ. Effects of dietary
monounsaturated fatty acids on lipoprotein concentrations,
compositions, and subfraction distributions and on VLDL
apolipoprotein B kinetics: dose-dependent effects on LDL. Am J Clin
Nutr. 2003 Jul;78(1):47-56. PMID:
12816770
112
Williams CM, Smith RD, Kelly CN, Fielding BA, Hauton D, Silva KD,
Nydahl MC, Miller GJ, Williams CM. Long-term monounsaturated
fatty acid diets reduce platelet aggregation in healthy young
subjects. Br J Nutr. 2003 Sep;90(3):597-607. PMID:
13129466
113
Ochoa JJ, Quiles JL, Ibanez S, Martinez E, Lopez-Frias M, Huertas
JR, Mataix J. Aging-related oxidative stress depends on dietary
lipid source in rat postmitotic tissues. J Bioenerg Biomembr. 2003
Jun;35(3):267-75. PMID:
13678277
114
Colette C, Percheron C, Pares-Herbute N, Michel F, Pham TC,
Brillant L, Descomps B, Monnier L. Exchanging carbohydrates for
monounsaturated fats in energy-restricted diets: effects on
metabolic profile and other cardiovascular risk factors. Int J Obes
Relat Metab Disord. 2003 Jun;27(6):648-56. PMID:
12833107
115
Perez-Jimenez F, Lopez-Miranda J, Mata P. Protective effect
of dietary monounsaturated fat on arteriosclerosis: beyond
cholesterol. Atherosclerosis. 2002 Aug;163(2):385-98. Review. PMID:
12052487
116
Faine LA, Diniz YS, Galhardi CM, Rodrigues HG, Burneiko RC,
Santana LS, Cicogna AC, Novelli EL. Synergistic action of olive
oil supplementation and dietary restriction on serum lipids and
cardiac antioxidant defences. Can J Physiol Pharmacol. 2004
Nov;82(11):969-975. PMID:
15644936
117
Solfrizzi V, D'Introno A, Colacicco AM, Capurso C, Palasciano R,
Capurso S, Torres F, Capurso A, Panza F. Unsaturated fatty acids
intake and all-causes mortality: a 8.5-year follow-up of the Italian
Longitudinal Study on Aging. Exp Gerontol. 2005 Apr;40(4):335-43.
PMID:
15820615
118
Dietary fatty acids and the risk of Parkinson disease: the Rotterdam
study. Neurology. 2005 Jun 28;64(12):2040-5. PMID:
15985568
119
van Gool CJ, Thijs C, Henquet CJ, van Houwelingen AC, Dagnelie
PC, Schrander J, Menheere PP, van den brandt PA. Gamma-linolenic
acid supplementation for prophylaxis of atopic dermatitis--a
randomized controlled trial in infants at high familial risk. Am J
Clin Nutr. 2003 Apr;77(4):943-51. PMID:
12663296
120
Seidman MD, Khan MJ, Tang WX, Quirk WS. Influence of lecithin
on mitochondrial DNA and age-related hearing loss. Otolaryngol Head
Neck Surg. 2002 Sep; 127(3): 138-44. PMID:
12297801
121
Lambert AJ, Merry BJ. Effect of Caloric Restriction on
Mitochondrial Reactive Oxygen Species Production and Bioenergetics -
REVERSAL BY INSULIN. Am J Physiol Regul Integr Comp Physiol. 2003
Sep 11 [Epub ahead of print] PMID:
12969875
122
Studer M, Briel M, Leimenstoll B, Glass TR, Bucher HC. Effect
of different antilipidemic agents and diets on mortality: a
systematic review. Arch Intern Med. 2005 Apr 11;165(7):725-30. PMID:
15824290
123
Laaksonen DE, Nyyssonen K, Niskanen L, Rissanen TH, Salonen JT.
Prediction of Cardiovascular Mortality in Middle-aged Men by Dietary
and Serum Linoleic and Polyunsaturated Fatty Acids. Arch Intern Med.
2005 Jan 24;165(2):193-9. PMID:
15668366
125
Melanson SF, Lewandrowski EL, Flood JG, Lewandrowski KB.
Measurement of organochlorines in commercial over-the-counter fish
oil preparations: implications for dietary and therapeutic
recommendations for omega-3 fatty acids and a review of the
literature. Arch Pathol Lab Med. 2005 Jan;129(1):74-7. PMID:
15628911
126
Iribarren C, Markovitz JH, Jacobs DR, Schreiner PJ, Daviglus M,
Hibbeln JR. Dietary intake of n-3, n-6 fatty acids and fish:
Relationship with hostility in young adults-the CARDIA study. Eur J
Clin Nutr. 2004 Jan; 58(1): 24-31. PMID:
14679363
127
Richardson AJ, Cyhlarova E, Ross MA. Omega-3 and omega-6
fatty acid concentrations in red blood cell membranes relate to
schizotypal traits in healthy adults. Prostaglandins Leukot Essent
Fatty Acids. 2003 Dec;69(6):461-6. PMID:
14623500
128
He K, Song Y, Daviglus ML, Liu K, Van Horn L, Dyer AR, Greenland
P. Accumulated evidence on fish consumption and coronary heart
disease mortality: a meta-analysis of cohort studies. Circulation.
2004 Jun 8;109(22):2705-11. PMID:
15184295
129
He K, Song Y, Daviglus ML, Liu K, Van Horn L, Dyer AR, Goldbourt
U, Greenland P. Fish consumption and incidence of stroke: a
meta-analysis of cohort studies. Stroke. 2004 Jul;35(7):1538-42.
Epub 2004 May 20. PMID:
15155968
130
Mozaffarian D, Longstreth WT Jr, Lemaitre RN, Manolio TA, Kuller
LH, Burke GL, Siscovick DS. Fish Consumption and Stroke Risk in
Elderly Individuals: The Cardiovascular Health Study. Arch Intern
Med. 2005 Jan 24;165(2):200-206. PMID:
15668367
131
Dallongeville J, Yarnell J, Ducimetiere P, Arveiler D, Ferrieres
J, Montaye M, Luc G, Evans A, Bingham A, Hass B, Ruidavets JB,
Amouyel P. Fish consumption is associated with lower heart
rates. Circulation. 2003 Aug 19;108(7):820-5. Epub 2003 Aug 11.
PMID:
12912821
133
Barberger-Gateau P, Letenneur L, Deschamps V, Peres K, Dartigues
JF, Renaud S. Fish, meat, and risk of dementia: cohort study.
BMJ. 2002 Oct 26;325(7370):932-3. PMID:
12399342
135
Augustsson K, Michaud DS, Rimm EB, Leitzmann MF, Stampfer MJ,
Willett WC, Giovannucci E. A prospective study of intake of fish
and marine fatty acids and prostate cancer. Cancer Epidemiol
Biomarkers Prev. 2003 Jan;12(1):64-7. PMID:
12540506
137
Cigarette Smoking, Fish Consumption, Omega-3 Fatty Acid Intake, and
Associations With Age-Related Macular Degeneration: The US Twin
Study of Age-Related Macular Degeneration. Arch Ophthalmol. 2006
Jul;124(7):995-1001. PMID:
16832023
138
Trichopoulou A, Costacou T, Bamia C, Trichopoulos D.
Adherence to a Mediterranean diet and survival in a Greek
population. N Engl J Med. 2003 Jun 26;348(26):2599-608. PMID:
12826634
139
Mediterranean diet, lifestyle factors, and 10-year mortality in
elderly European men and women: the HALE project. JAMA. 2004 Sep
22;292(12):1433-9. PMID:
15383513
140
Mediterranean diet and risk for Alzheimer's disease. Ann Neurol.
2006 Apr 18; PMID:
16622828
141
Ravaglia G, Forti P, Maioli F, Muscari A, Sacchetti L, Arnone G,
Nativio V, Talerico T, Mariani E. Homocysteine and cognitive
function in healthy elderly community dwellers in Italy. Am J Clin
Nutr. 2003 Mar;77(3):668-73. PMID:
12600859
143
Ganji V, Kafai MR. Demographic, health, lifestyle, and blood
vitamin determinants of serum total homocysteine concentrations in
the third National Health and Nutrition Examination Survey,
1988-1994. Am J Clin Nutr. 2003 Apr;77(4):826-33. PMID:
12663279
146
van Oort FV, Melse-Boonstra A, Brouwer IA, Clarke R, West CE,
Katan MB, Verhoef P. Folic acid and reduction of plasma
homocysteine concentrations in older adults: a dose-response study.
Am J Clin Nutr. 2003 May;77(5):1318-23. PMID:
12716688
147
Atzmon G, Gabriely I, Greiner W, Davidson D, Schechter C,
Barzilai N. Plasma HDL levels highly correlate with cognitive
function in exceptional longevity. J Gerontol A Biol Sci Med Sci.
2002 Nov;57(11):M712-5. PMID:
12403798
148
Bittner V. Non-high-density lipoprotein cholesterol and
cardiovascular disease. Curr Opin Lipidol. 2003 Aug;14(4):367-71.
PMID:
12865734
149
Nissen SE, Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA,
Crowe T, Howard G, Cooper CJ, Brodie B, Grines CL, DeMaria AN;
REVERSAL Investigators. Effect of intensive compared with
moderate lipid-lowering therapy on progression of coronary
atherosclerosis: a randomized controlled trial. JAMA. 2004 Mar
3;291(9):1071-80. PMID:
14996776
150
Jenkins DJ, Kendall CW, Marchie A, Faulkner DA, Wong JM, de Souza
R, Emam A, Parker TL, Vidgen E, Lapsley KG, Trautwein EA, Josse RG,
Leiter LA, Connelly PW. Effects of a dietary portfolio of
cholesterol-lowering foods vs lovastatin on serum lipids and
C-reactive protein. JAMA. 2003 Jul 23;290(4):502-10. PMID:
12876093
151
Jenkins DJ, Kendall CW, Marchie A, Faulkner DA, Wong JM, de Souza
R, Emam A, Parker TL, Vidgen E, Trautwein EA, Lapsley KG, Josse RG,
Leiter LA, Singer W, Connelly PW. Direct comparison of a dietary
portfolio of cholesterol-lowering foods with a statin in
hypercholesterolemic participants. Am J Clin Nutr. 2005
Feb;81(2):380-7. PMID:
15699225
152
Sacks FM. Dietary phytoestrogens to prevent cardiovascular
disease: early promise unfulfilled. Circulation. 2005 Feb
1;111(4):385-7. No abstract available. PMID: 15687122
154
McGwin G Jr, McNeal S, Owsley C, Girkin C, Epstein D, Lee PP.
Statins and other cholesterol-lowering medications and the
presence of glaucoma. Arch Ophthalmol. 2004 Jun;122(6):822-6. PMID:
15197056
155
Liu S, Sesso HD, Manson JE, Willett WC, Buring JE. Is intake
of breakfast cereals related to total and cause-specific mortality
in men? Am J Clin Nutr. 2003 Mar;77(3):594-9. PMID:
12600848
156
Montonen J, Knekt P, Jarvinen R, Aromaa A, Reunanen A.
Whole-grain and fiber intake and the incidence of type 2
diabetes. Am J Clin Nutr. 2003 Mar;77(3):622-9. PMID:
12600852
157
McIntosh GH, Noakes M, Royle PJ, Foster PR. Whole-grain rye
and wheat foods and markers of bowel health in overweight
middle-aged men. Am J Clin Nutr. 2003 Apr;77(4):967-74. PMID:
12663299
158
Montonen J, Knekt P, Jarvinen R, Aromaa A, Reunanen A.
Whole-grain and fiber intake and the incidence of type 2
diabetes. Am J Clin Nutr. 2003 Mar;77(3):622-9. PMID:
12600852
159
Whole-grain intake is inversely associated with the metabolic
syndrome and mortality in older adults. Am J Clin Nutr. 2006
Jan;83(1):124-31. PMID:
16400060
161
Fung TT, Hu FB, Pereira MA, Liu S, Stampfer MJ, Colditz GA,
Willett WC. Whole-grain intake and the risk of type 2 diabetes:
a prospective study in men. Am J Clin Nutr. 2002 Sep;76(3):535-40.
PMID:
12197996
162
Whole-grain and fiber intakes and periodontitis risk in men. Am J
Clin Nutr. 2006 Jun;83(6):1395-400. PMID:
16762952
164
Effect of an oat bran enriched diet on the atherogenic lipid profile
in patients with an increased coronary heart disease risk. A
controlled randomized lifestyle intervention study. Ann Nutr Metab.
2003;47(6):306-11. PMID:
14520027
165
Effect of an oat bran-rich supplement on the metabolic profile of
overweight premenopausal women. Ann Nutr Metab. 2005
May-Jun;49(3):141-8. Epub 2005 May 24. PMID:
15942159
166
Vanharanta M, Voutilainen S, Rissanen TH, Adlercreutz H, Salonen
JT. Risk of cardiovascular disease-related and all-cause death
according to serum concentrations of enterolactone: Kuopio Ischaemic
Heart Disease Risk Factor Study. Arch Intern Med. 2003 May
12;163(9):1099-104. PMID:
12742810
167
Tarpila S, Aro A, Salminen I, Tarpila A, Kleemola P, Akkila J,
Adlercreutz H. The effect of flaxseed supplementation in
processed foods on serum fatty acids and enterolactone. Eur J Clin
Nutr. 2002 Feb;56(2):157-65. PMID:
11857049
168
Bhathena SJ, Ali AA, Haudenschild C, Latham P, Ranich T, Mohamed
AI, Hansen CT, Velasquez MT. Dietary Flaxseed Meal is More
Protective Than Soy Protein Concentrate Against Hypertriglyceridemia
and Steatosis of the Liver in an Animal Model of Obesity. J Am Coll
Nutr. 2003 Apr;22(2):157-64. PMID:
12672712 (USDA study)
169
Lee IM, Sesso HD, Oguma Y, Paffenbarger RS Jr. Relative
intensity of physical activity and risk of coronary heart disease.
Circulation. 2003 Mar 4;107(8):1110-6. PMID:
12615787
170
Kurl S, Laukkanen JA, Rauramaa R, Lakka TA, Sivenius J, Salonen
JT. Cardiorespiratory fitness and the risk for stroke in men.
Arch Intern Med. 2003 Jul 28;163(14):1682-8. PMID:
12885683
172
Hu G, Barengo NC, Tuomilehto J, Lakka TA, Nissinen A, Jousilahti
P. Relationship of Physical Activity and Body Mass Index to the
Risk of Hypertension: A Prospective Study in Finland. Hypertension.
2004 Jan;43(1):25-30. Epub 2003 Dec 01. PMID:
14656958
173
Lee CD, Folsom AR, Blair SN. Physical activity and stroke
risk: a meta-analysis. Stroke. 2003 Oct;34(10):2475-81. Epub 2003
Sep 18. PMID:
14500932
174
Holloszy JO. Longevity of exercising male rats: effect of an
antioxidant supplemented diet. Mech Ageing Dev. 1998 Feb
16;100(3):211-9. PMID:
9578110
175
Holloszy JO. Mortality rate and longevity of food-restricted
exercising male rats: a reevaluation. J Appl Physiol. 1997
Feb;82(2):399-403. PMID:
9049716
176
Chang-Claude J, Hermann S, Eilber U, Steindorf K. Lifestyle
determinants and mortality in German vegetarians and
health-conscious persons: results of a 21-year follow-up. Cancer
Epidemiol Biomarkers Prev. 2005 Apr;14(4):963-8. PMID:
15824171
177
Pimentel AE, Gentile CL, Tanaka H, Seals DR, Gates PE. Greater
rate of decline in maximal aerobic capacity with age in
endurance-trained than in sedentary men. J Appl Physiol. 2003
Jun;94(6):2406-13. Epub 2003 Jan 17. PMID:
12533496
178
Ross R, Janssen I, Dawson J, Kungl AM, Kuk JL, Wong SL,
Nguyen-Duy TB, Lee S, Kilpatrick K, Hudson R. Exercise-induced
reduction in obesity and insulin resistance in women: a randomized
controlled trial. Obes Res. 2004 May;12(5):789-98. PMID:
15166299
179
Leisure-time physical activity at midlife and the risk of dementia
and Alzheimer's disease. Lancet Neurol. 2005 Nov;4(11):705-11. PMID:
16239176
180
Exercise is associated with reduced risk for incident dementia among
persons 65 years of age and older. Ann Intern Med. 2006 Jan
17;144(2):73-81. PMID:
16418406
181
Physical Activity and the 15-year Cumulative Incidence of
Age-related Macular Degeneration: The Beaver Dam Eye Study. Br J
Ophthalmol. 2006 Oct 31; PMID:
17077116
182
Physical activity and risk of colon and rectal cancers: the European
prospective investigation into cancer and nutrition. Cancer
Epidemiol Biomarkers Prev. 2006 Dec;15(12):2398-407. PMID:
17164362
183
Avisar R, Avisar E, Weinberger D. Effect of coffee
consumption on intraocular pressure. Ann Pharmacother. 2002
Jun;36(6):992-5. PMID:
12022898
184
Maia L, de Mendonca A. Does caffeine intake protect from
Alzheimer's disease? Eur J Neurol. 2002 Jul;9(4):377-82. PMID:
12099922
185
Negishi H, Xu JW, Ikeda K, Njelekela M, Nara Y, Yamori Y. Black
and Green Tea Polyphenols Attenuate Blood Pressure Increases in
Stroke-Prone Spontaneously Hypertensive Rats. J Nutr. 2004
Jan;134(1):38-42. PMID:
14704290
186
Yang YC, Lu FH, Wu JS, Wu CH, Chang CJ. The protective effect
of habitual tea consumption on hypertension. Arch Intern Med. 2004
Jul 26;164(14):1534-40. PMID:
15277285
187
Addition of milk prevents vascular protective effects of tea. Eur
Heart J. 2007 Jan 9; PMID:
17213230
188
Jankun J, Selman SH, Swiercz R, Skrzypczak-Jankun E. Why
drinking green tea could prevent cancer. Nature. 1997 Jun
5;387(6633):561. No abstract available. PMID: 9177339
190
Wu AH, Yu MC, Tseng CC, Hankin J, Pike MC. Green tea and risk
of breast cancer in Asian Americans. Int J Cancer. 2003 Sep
10;106(4):574-9. PMID:
12845655
193
Panagiotakos DB, Pitsavos C, Chrysohoou C, Kokkinos P, Toutouzas
P, Stefanadis C. The J-shaped effect of coffee consumption on
the risk of developing acute coronary syndromes: the CARDIO2000
case-control study. J Nutr. 2003 Oct;133(10):3228-32. PMID:
14519815
194
Consumption of coffee is associated with reduced risk of death
attributed to inflammatory and cardiovascular diseases in the Iowa
Women's Health Study. Am J Clin Nutr. 2006 May;83(5):1039-46. PMID:
16685044
195
Rust J. Coffee intake over 33 years is not associated with
developing hypertension. J Clin Hypertens (Greenwich). 2002
Nov-Dec;4(6):434. No abstract available. PMID: 12461309
196
Habitual caffeine intake and the risk of hypertension in women.
JAMA. 2005 Nov 9;294(18):2330-5. PMID:
16278361
197
Verhoef P, Pasman WJ, Van Vliet T, Urgert R, Katan MB.
Contribution of caffeine to the homocysteine-raising effect of
coffee: a randomized controlled trial in humans. Am J Clin Nutr.
2002 Dec;76(6):1244-8. PMID:
12450889
198
Iwai N, Ohshiro H, Kurozawa Y, Hosoda T, Morita H, Funakawa K,
Okamoto M, Nose T. Relationship between coffee and green tea
consumption and all-cause mortality in a cohort of a rural Japanese
population. J Epidemiol. 2002 May;12(3):191-8. PMID:
12164320
199
Rosengren A, Dotevall A, Wilhelmsen L, Thelle D, Johansson S.
Coffee and incidence of diabetes in Swedish women: a prospective
18-year follow-up study. J Intern Med. 2004 Jan;255(1):89-95. PMID:
14687243
200
van Dam RM, Feskens EJ. Coffee consumption and risk of type 2
diabetes mellitus. Lancet. 2002 Nov 9;360(9344):1477-8. PMID:
12433517
201
Salazar-Martinez E, Willett WC, Ascherio A, Manson JE, Leitzmann
MF, Stampfer MJ, Hu FB. Coffee consumption and risk for type 2
diabetes mellitus. Ann Intern Med. 2004 Jan 6;140(1):1-8. PMID:
14706966
202
Tuomilehto J, Hu G, Bidel S, Lindstrom J, Jousilahti P. Coffee
consumption and risk of type 2 diabetes mellitus among middle-aged
Finnish men and women. JAMA. 2004 Mar 10;291(10):1213-9. PMID:
15010442
203
Coffee consumption and risk of type 2 diabetes: a systematic review.
JAMA. 2005 Jul 6;294(1):97-104. PMID:
15998896
204
Consumption of coffee, but not black tea, is associated with
decreased risk of premenopausal breast cancer. J Nutr. 2006
Jan;136(1):166-71. PMID:
16365077
205
Carbonated soft drink consumption and risk of esophageal
adenocarcinoma. J Natl Cancer Inst. 2006 Jan 4;98(1):72-5. PMID:
16391374
207
CR society post, 2006-04-09
208
Lagiou P, Samoli E, Lagiou A, Tzonou A, Kalandidi A, Peterson J,
Dwyer J, Trichopoulos D. Intake of specific flavonoid classes
and coronary heart disease-a case-control study in Greece. Eur J
Clin Nutr. 2004 Dec;58(12):1643-1648. PMID:
15226759
210
Lee CK, Pugh TD, Klopp RG, Edwards J, Allison DB, Weindruch R,
Prolla TA. The impact of alpha-lipoic acid, coenzyme Q10 and
caloric restriction on life span and gene expression patterns in
mice. Free Radic Biol Med. 2004 Apr 15;36(8):1043-57. PMID:
15059645
211
Dietary intake of antioxidants and risk of age-related macular
degeneration. JAMA. 2005 Dec 28;294(24):3101-7. PMID:
16380590
213
Brown MJ, Ferruzzi MG, Nguyen ML, Cooper DA, Eldridge AL,
Schwartz SJ, White WS. Carotenoid bioavailability is higher from
salads ingested with full-fat than with fat-reduced salad dressings
as measured with electrochemical detection. Am J Clin Nutr. 2004
Aug;80(2):396-403. PMID:
15277161
214
Vegetable Intake and Long-term Survival among Middle-aged Men in
Italy. Ann Epidemiol 2003;13:424–430.s
215
Associations of vegetable and fruit consumption with age-related
cognitive change. Neurology. 2006 Oct 24;67(8):1370-6. PMID:
17060562
216
Siener R, Hesse A. The effect of a vegetarian and different
omnivorous diets on urinary risk factors for uric acid stone
formation. Eur J Nutr. 2003 Dec;42(6):332-7. PMID:
14673606
218
Joseph JA, Denisova NA, Bielinski D, Fisher DR, Shukitt-Hale B.
Oxidative stress protection and vulnerability in aging: putative
nutritional implications for intervention. Mech Ageing Dev. 2000 Jul
31;116(2-3):141-53. Review. PMID:
10996014
219
Milgram NW, Head E, Zicker SC, Ikeda-Douglas CJ, Murphey H,
Muggenburg B, Siwak C, Tapp D, Cotman CW. Learning ability in
aged beagle dogs is preserved by behavioral enrichment and dietary
fortification: a two-year longitudinal study. Neurobiol Aging. 2005
Jan;26(1):77-90. PMID:
15585348
220
Djousse L, Arnett DK, Coon H, Province MA, Moore LL, Ellison RC.
Fruit and vegetable consumption and LDL cholesterol: the
National Heart, Lung, and Blood Institute Family Heart Study. Am J
Clin Nutr. 2004 Feb;79(2):213-7. PMID:
14749225
221
Tylavsky FA, Holliday K, Danish R, Womack C, Norwood J, Carbone
L. Fruit and vegetable intakes are an independent predictor of
bone size in early pubertal children. Am J Clin Nutr. 2004
Feb;79(2):311-7. PMID:
14749239
222
Hung HC, Joshipura KJ, Jiang R, Hu FB, Hunter D, Smith-Warner SA,
Colditz GA, Rosner B, Spiegelman D, Willett WC. Fruit and
vegetable intake and risk of major chronic disease. J Natl Cancer
Inst. 2004 Nov 3;96(21):1577-84. PMID:
15523086
223
Schwenke DC. Insulin resistance, low-fat diets, and
low-carbohydrate diets: time to test new menus. Curr Opin Lipidol.
2005 Feb;16(1):55-60. PMID:
15650564
224
A 4-wk intervention with high intake of carotenoid-rich vegetables
and fruit reduces plasma C-reactive protein in healthy, nonsmoking
men. Am J Clin Nutr. 2005 Nov;82(5):1052-8. PMID:
16280438
225
Fruit and vegetable consumption and risk of stroke: a meta-analysis
of cohort studies. Neurology. 2005 Oct 25;65(8):1193-7. PMID:
16247045
226
Fruit and vegetable consumption and stroke: meta-analysis of cohort
studies. Lancet. 2006 Jan 28;367(9507):320-6. PMID:
16443039
227
Association between fruit and vegetable consumption and oral cancer:
a meta-analysis of observational studies. Am J Clin Nutr. 2006
May;83(5):1126-1134. PMID:
16685056
228
Fruit and Vegetable Consumption and Risk of Coronary Heart Disease:
A Meta-Analysis of Cohort Studies. J Nutr. 2006
Oct;136(10):2588-2593. PMID:
16988131
231
N. V. Matusheski and E. H. JEFFERY. Processing conditions improve
the yield of the anticarcinogen sulforaphane from broccoli.
Department of Food Science and Human Nutrition, University of
Illinois Institute of Food Technology 2002 Annual Meeting. Abstract
232
Wu L, Ashraf MH, Facci M, Wang R, Paterson PG, Ferrie A, Juurlink
BH. Dietary approach to attenuate oxidative stress,
hypertension, and inflammation in the cardiovascular system. Proc
Natl Acad Sci U S A. 2004 May 4;101(18):7094-9. Epub 2004 Apr 21.
PMID:
15103025
233
Kang JH, Ascherio A, Grodstein F. Fruit and vegetable
consumption and cognitive decline in aging women. Ann Neurol. 2005
Apr 25;57(5):713-720 [Epub ahead of print] PMID:
15852398
234
Hsing AW, Chokkalingam AP, Gao YT, Madigan MP, Deng J, Gridley G,
Fraumeni JF Jr. Allium vegetables and risk of prostate cancer:
a population-based study. J Natl Cancer Inst. 2002 Nov
6;94(21):1648-51. PMID:
12419792
235
Josling P. Preventing the common cold with a garlic
supplement: a double-blind, placebo-controlled survey. Adv Ther.
2001 Jul-Aug;18(4):189-93. PMID:
11697022
236
Lopez-Carrillo L, Lopez-Cervantes M, Robles-Diaz G,
Ramirez-Espitia A, Mohar-Betancourt A, Meneses-Garcia A, Lopez-Vidal
Y, Blair A. Capsaicin consumption, Helicobacter pylori
positivity and gastric cancer in Mexico. Int J Cancer. 2003 Aug
20;106(2):277-82. PMID:
12800206
237
Mozaffarieh M, Sacu S, Wedrich A. The role of the
carotenoids, lutein and zeaxanthin, in protecting against
age-related macular degeneration: A review based on controversial
evidence. Nutr J. 2003 Dec 11;2(1):20. PMID:
14670087 http://www.nutritionj.com/content/2/1/20
(free full text)
238
Lutein and zeaxanthin intakes and risk of age-related macular
degeneration and cataracts: an evaluation using the Food and Drug
Administration's evidence-based review system for health claims. Am
J Clin Nutr. 2006 Nov;84(5):971-4. PMID:
17093145
239
Jian L, Du CJ, Lee AH, Binns CW. Do dietary lycopene and
other carotenoids protect against prostate cancer? Int J Cancer.
2004 Oct 28;113(6):1010-1014 PMID:
15514967
241
Pereira MA, O'Reilly E, Augustsson K, Fraser GE, Goldbourt U,
Heitmann BL, Hallmans G, Knekt P, Liu S, Pietinen P, Spiegelman D,
Stevens J, Virtamo J, Willett WC, Ascherio A. Dietary fiber and
risk of coronary heart disease: a pooled analysis of cohort studies.
Arch Intern Med. 2004 Feb 23;164(4):370-6. PMID:
14980987,
http://archinte.ama-assn.org/cgi/content/abstract/164/4/370
242
Kurowska EM, Manthey JA. Hypolipidemic effects and
absorption of citrus polymethoxylated flavones in hamsters with
diet-induced hypercholesterolemia. J Agric Food Chem. 2004 May
19;52(10):2879-86. PMID:
15137829
244
Hakim IA, Harris RB, Ritenbaugh C. Citrus peel use is
associated with reduced risk of squamous cell carcinoma of the skin.
Nutr Cancer. 2000;37(2):161-8. PMID:
11142088
245
Crowell PL. Prevention and therapy of cancer by dietary
monoterpenes. J Nutr. 1999 Mar;129(3):775S-778S. Review. PMID:
10082788
247
Key TJ, Fraser GE, Thorogood M, Appleby PN, Beral V, Reeves G,
Burr ML, Chang-Claude J, Frentzel-Beyme R, Kuzma JW, Mann J,
McPherson K. Mortality in vegetarians and nonvegetarians:
detailed findings from a collaborative analysis of 5 prospective
studies. Am J Clin Nutr. 1999 Sep;70(3 Suppl):516S-524S. PMID:
10479225
249
Chang-Claude J, Hermann S, Eilber U, Steindorf K. Lifestyle
determinants and mortality in German vegetarians and
health-conscious persons: results of a 21-year follow-up. Cancer
Epidemiol Biomarkers Prev. 2005 Apr;14(4):963-8. PMID:
15824171
250
Cho E, Seddon JM, Rosner B, Willett WC, Hankinson SE. Prospective
study of intake of fruits, vegetables, vitamins, and carotenoids and
risk of age-related maculopathy. Arch Ophthalmol. 2004
Jun;122(6):883-92. PMID:
15197064
251
Fruit and vegetable juices and Alzheimer's disease: the Kame
Project. Am J Med. 2006 Sep;119(9):751-9. PMID:
16945610
252
Joseph JA, Shukitt-Hale B, Denisova NA, Bielinski D, Martin A,
McEwen JJ, Bickford PC. Reversals of age-related declines in
neuronal signal transduction, cognitive, and motor behavioral
deficits with blueberry, spinach, or strawberry dietary
supplementation. J Neurosci. 1999 Sep 15;19(18):8114-21.PMID:
10479711
253
R. Martin, R.J. Coppings, K.E. Gerstmann, J.A. Joseph, A.C. Kokesh,
B. Kristal, D. Mathew, B. Sachs, A. Pruchnicki, R. Schnoll, A.
Wetherell. THE 2002 BLUEBERRY HEALTH STUDY: DAILY BLUEBERRIES
IMPROVE DECISION-SPEED AND AGE-RELATED HEALTH INDICATORS.
http://www.americanaging.org/past_meetings/AGE03/abs/Martin.htm.
254
Boileau TW, Liao Z, Kim S, Lemeshow S, Erdman JW Jr, Clinton SK.
Prostate carcinogenesis in N-methyl-N-nitrosourea
(NMU)-testosterone-treated rats fed tomato powder, lycopene, or
energy-restricted diets. J Natl Cancer Inst. 2003 Nov
5;95(21):1578-86. PMID:
14600090
255
Pomegranate juice consumption for 3 years by patients with carotid
artery stenosis reduces common carotid intima-media thickness, blood
pressure and LDL oxidation. Clin Nutr. 2004 Jun;23(3):423-33. PMID:
15158307
256
Effects of pomegranate juice consumption on myocardial perfusion in
patients with coronary heart disease. Am J Cardiol. 2005 Sep
15;96(6):810-4. PMID:
16169367
258
Legumes: the most important dietary predictor of survival in older
people of different ethnicities. Asia Pac J Clin Nutr.
2004;13(Suppl):S126. PMID:
15294666
259
Vegetables, fruits, legumes and prostate cancer: a multiethnic
case-control study. Cancer Epidemiol Biomarkers Prev. 2000
Aug;9(8):795-804. PMID:
10952096
260
Mukamal KJ, Kuller LH, Fitzpatrick AL, Longstreth WT Jr,
Mittleman MA, Siscovick DS. Prospective study of alcohol
consumption and risk of dementia in older adults. JAMA. 2003 Mar
19;289(11):1405-13. PMID:
12636463
261
Anttila T, Helkala EL, Viitanen M, Kareholt I, Fratiglioni L,
Winblad B, Soininen H, Tuomilehto J, Nissinen A, Kivipelto M.
Alcohol drinking in middle age and subsequent risk of mild cognitive
impairment and dementia in old age: a prospective population based
study. BMJ. 2004 Sep 4;329(7465):539. Epub 2004 Aug 10. PMID:
15304383
Larrieu S, Letenneur L, Helmer C, Dartigues JF,
Barberger-Gateau P. Nutritional factors and risk of incident
dementia in the PAQUID longitudinal cohort. J Nutr Health Aging.
2004;8(3):150-4. PMID: 15129300
Luchsinger JA, Tang MX,
Siddiqui M, Shea S, Mayeux R. Alcohol intake and risk of
dementia. J Am Geriatr Soc. 2004 Apr;52(4):540-6. PMID: 15066068
Letenneur L, Larrieu S, Barberger-Gateau P. Alcohol and
tobacco consumption as risk factors of dementia: a review of
epidemiological studies. Biomed Pharmacother. 2004 Mar;58(2):95-9.
Review. PMID: 14992790
Truelsen T, Thudium D, Gronbaek M;
Copenhagen City Heart Study. Amount and type of alcohol and risk of
dementia: the Copenhagen City Heart Study. Neurology. 2002 Nov
12;59(9):1313-9. PMID: 12427876
Schlienger JL.
[Beneficial and deleterious effects of alcoholic beverages] Rev
Prat. 1999 Feb 15;49(4):367-72. Review. French. PMID: 10319684
Leibovici D, Ritchie K, Ledesert B, Touchon J. The
effects of wine and tobacco consumption on cognitive performance in
the elderly: a longitudinal study of relative risk. Int J Epidemiol.
1999 Feb;28(1):77-81. PMID: 10195668
Orgogozo
JM, Dartigues JF, Lafont S, Letenneur L, Commenges D, Salamon R,
Renaud S, Breteler MB. Wine consumption and dementia in the
elderly: a prospective community study in the Bordeaux area. Rev
Neurol (Paris). 1997 Apr;153(3):185-92. PMID: 9296132
Galanis
DJ, Joseph C, Masaki KH, Petrovitch H, Ross GW, White L. A
longitudinal study of drinking and cognitive performance in elderly
Japanese American men: the Honolulu-Asia Aging Study. Am J Public
Health. 2000 Aug;90(8):1254-9. PMID: 10937006
Leroi I,
Sheppard JM, Lyketsos CG. Cognitive function after 11.5 years of
alcohol use: relation to alcohol use. Am J Epidemiol. 2002 Oct
15;156(8):747-52. PMID: 12370163
Ruitenberg A, van Swieten
JC, Witteman JC, Mehta KM, van Duijn CM, Hofman A, Breteler MM.
Alcohol consumption and risk of dementia: the Rotterdam Study.
Lancet. 2002 Jan 26;359(9303):281-6. PMID: 11830193
Huang W,
Qiu C, Winblad B, Fratiglioni L. Alcohol consumption and
incidence of dementia in a community sample aged 75 years and older.
J Clin Epidemiol. 2002 Oct;55(10):959-64. PMID: 12464371
262
Stampfer MJ, Kang JH, Chen J, Cherry R, Grodstein F. Effects
of Moderate Alcohol Consumption on Cognitive Function in Women. N
Engl J Med. 2005 Jan 20;352(3):245-253. PMID:
15659724
263
Moderate Alcohol Consumption Reduces Risk of Ischemic Stroke. The
Northern Manhattan Study. Stroke. 2005 Nov 23; [Epub ahead of print]
PMID:
16306464
264
Malinski MK, Sesso HD, Lopez-Jimenez F, Buring JE, Gaziano JM.
Alcohol consumption and cardiovascular disease mortality in
hypertensive men. Arch Intern Med. 2004 Mar 22;164(6):623-8. PMID:
15037490
265
Vliegenthart R, Oei HH, van den Elzen AP, van Rooij FJ, Hofman A,
Oudkerk M, Witteman JC. Alcohol consumption and coronary
calcification in a general population. Arch Intern Med. 2004 Nov
22;164(21):2355-60. PMID:
15557415
266
Arndt V, Rothenbacher D, Krauledat R, Daniel U, Brenner H. Age,
alcohol consumption, and all-cause mortality. Ann Epidemiol. 2004
Nov;14(10):750-3. PMID:
15519897
267
Doll R, Peto R, Boreham J, Sutherland I. Mortality in
relation to alcohol consumption: a prospective study among male
British doctors. Int J Epidemiol. 2005 Jan 12; [Epub ahead of print]
PMID:
15647313
268
Alcohol dosing and total mortality in men and women: An updated
meta-analysis of 34 prospective studies. Arch Intern Med. 2006 Dec
11-25;166(22):2437-45. PMID:
17159008
269
Hamajima N, Hirose K, Tajima K, et al. Alcohol, tobacco and
breast cancer--collaborative reanalysis of individual data from 53
epidemiological studies, including 58,515 women with breast cancer
and 95,067 women without the disease. Br J Cancer. 2002 Nov
18;87(11):1234-45. PMID:
12439712
270
Stranges S, Wu T, Dorn JM, Freudenheim JL, Muti P, Farinaro E,
Russell M, Nochajski TH, Trevisan M. Relationship of Alcohol
Drinking Pattern to Risk of Hypertension. A Population-Based Study.
Hypertension. 2004 Oct 11; [Epub ahead of print] PMID:
15477381
271
Zilkens RR, Burke V, Hodgson JM, Barden A, Beilin LJ, Puddey IB.
Red wine and beer elevate blood pressure in normotensive men.
Hypertension. 2005 May;45(5):874-9. Epub 2005 Apr 18. PMID:
15837829
272
Alcohol consumption and risk for coronary heart disease among men
with hypertension. Ann Intern Med. 2007 Jan 2;146(1):10-9. PMID:
17200217
273
Schoonen WM, Salinas CA, Kiemeney LA, Stanford JL. Alcohol
consumption and risk of prostate cancer in middle-aged men. Int J
Cancer. 2005 Jan 1;113(1):133-40. PMID:
15386436
274
Resveratrol improves health and survival of mice on a high-calorie
diet. Nature. 2006 Nov 1; PMID:
17086191
275
Chen HL, Sheu WH, Tai TS, Liaw YP, Chen YC. Konjac supplement
alleviated hypercholesterolemia and hyperglycemia in type 2 diabetic
subjects--a randomized double-blind trial. J Am Coll Nutr. 2003
Feb;22(1):36-42. PMID:
12569112
276
Vuksan V, Sievenpiper JL, Owen R, Swilley JA, Spadafora P,
Jenkins DJ, Vidgen E, Brighenti F, Josse RG, Leiter LA, Xu Z,
Novokmet R. Beneficial effects of viscous dietary fiber from
Konjac-mannan in subjects with the insulin resistance syndrome:
results of a controlled metabolic trial. Diabetes Care. 2000
Jan;23(1):9-14. PMID:
10857960
277
Rigaud D, Paycha F, Meulemans A, Merrouche M, Mignon M. Effect
of psyllium on gastric emptying, hunger feeling and food intake in
normal volunteers: a double blind study. Eur J Clin Nutr. 1998
Apr;52(4):239-45. PMID:
9578335
278
Wu H, Dwyer KM, Fan Z, Shircore A, Fan J, Dwyer JH. Dietary
fiber and progression of atherosclerosis: the Los Angeles
Atherosclerosis Study. Am J Clin Nutr. 2003 Dec;78(6):1085-91. PMID:
14668268
279
Uusitupa M, Aro A, Korhonen T, Tuunainen A, Sarlund H, Penttila
I. Blood glucose and serum insulin responses to breakfast
including guar gum and cooked or uncooked milk in type 2
(non-insulin-dependent) diabetic patients. Diabetologia. 1984
Jun;26(6):453-5. PMID:
6088333
280
Wolever TM, Vuksan V, Eshuis H, Spadafora P, Peterson RD, Chao
ES, Storey ML, Jenkins DJ. Effect of method of administration of
psyllium on glycemic response and carbohydrate digestibility. J Am
Coll Nutr. 1991 Aug;10(4):364-71. PMID:
1654354
281
Chandalia M, Garg A, Lutjohann D, von Bergmann K, Grundy SM,
Brinkley LJ. Beneficial effects of high dietary fiber intake in
patients with type 2 diabetes mellitus. N Engl J Med. 2000 May
11;342(19):1392-8. PMID:
10805824
282
Pins JJ, Geleva D, Keenan JM, Frazel C, O'Connor PJ, Cherney LM.
Do whole-grain oat cereals reduce the need for antihypertensive
medications and improve blood pressure control? J Fam Pract. 2002
Apr;51(4):353-9. PMID:
11978259
283
Jenkins DJ, Kendall CW, Popovich DG, Vidgen E, Mehling CC, Vuksan
V, Ransom TP, Rao AV, Rosenberg-Zand R, Tariq N, Corey P, Jones PJ,
Raeini M, Story JA, Furumoto EJ, Illingworth DR, Pappu AS, Connelly
PW. Effect of a very-high-fiber vegetable, fruit, and nut diet
on serum lipids and colonic function. Metabolism. 2001
Apr;50(4):494-503. PMID:
11288049
284
Ajani UA, Ford ES, Mokdad AH. Dietary fiber and C-reactive
protein: findings from national health and nutrition examination
survey data. J Nutr. 2004 May;134(5):1181-5. PMID:
15113967
285
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R;
Prospective Studies Collaboration. Age-specific relevance of
usual blood pressure to vascular mortality: a meta-analysis of
individual data for one million adults in 61 prospective studies.
Lancet. 2002 Dec 14;360(9349):1903-13. PMID:
12493255
286
Hansen TW, Jeppesen J, Rasmussen S, Ibsen H, Torp-Pedersen C.
Ambulatory blood pressure and mortality: a population-based study.
Hypertension. 2005 Apr;45(4):499-504. Epub 2005 Mar 7. PMID:
15753229
288
Elias PK, Elias MF, Robbins MA, Budge MM. Blood
pressure-related cognitive decline: does age make a difference?
Hypertension. 2004 Nov;44(5):631-6. Epub 2004 Oct 04. PMID:
15466661
289
van Dijk EJ, Breteler MM, Schmidt R, Berger K, Nilsson LG,
Oudkerk M, Pajak A, Sans S, de Ridder M, Dufouil C, Fuhrer R,
Giampaoli S, Launer LJ, Hofman A. The association between blood
pressure, hypertension, and cerebral white matter lesions:
cardiovascular determinants of dementia study. Hypertension. 2004
Nov;44(5):625-30. Epub 2004 Oct 04. PMID:
15466662
290
Kuo HK, Sorond F, Iloputaife I, Gagnon M, Milberg W, Lipsitz LA.
Effect of blood pressure on cognitive functions in elderly persons.
J Gerontol A Biol Sci Med Sci. 2004 Nov;59(11):1191-4. PMID:
15602074
291
Reducing the Risk of Dementia. Efficacy of Long-Term Treatment of
Hypertension. Stroke. 2006 Apr 6; PMID:
16601212
293
Exercise and blood pressure: applying findings from the laboratory
to the community setting. Clin Exp Pharmacol Physiol. 2006
Sep;33(9):868-71. PMID:
16922823
294
He FJ, MacGregor GA. How Far Should Salt Intake Be Reduced?
Hypertension. 2003 Nov 10 [Epub ahead of print] PMID:
14610100
296
Tsugane S, Sasazuki S, Kobayashi M, Sasaki S. Salt and salted
food intake and subsequent risk of gastric cancer among middle-aged
Japanese men and women. Br J Cancer. 2004 Jan 12;90(1):128-34. PMID:
14710219
297
Importance of Salt in Determining Blood Pressure in Children:
Meta-Analysis of Controlled Trials. Hypertension. 2006
Nov;48(5):861-869. Epub 2006 Sep 25. PMID:
17000923
298
Geleijnse JM, Kok FJ, Grobbee DE. Blood pressure response to
changes in sodium and potassium intake: a metaregression analysis of
randomised trials. J Hum Hypertens. 2003 Jul;17(7):471-80. PMID:
12821954
299
Slama M, Susic D, Frohlich ED. Prevention of hypertension.
Curr Opin Cardiol. 2002 Sep;17(5):531-6. Review. PMID:
12357131
300
He FJ, Markandu ND, Coltart R, Barron J, Macgregor GA. Effect
of Short-Term Supplementation of Potassium Chloride and Potassium
Citrate on Blood Pressure in Hypertensives. Hypertension. 2005
Apr;45(4):571-574. Epub 2005 Feb 21. PMID:
15723964
301
Effect of potassium-enriched salt on cardiovascular mortality and
medical expenses of elderly men. Am J Clin Nutr. 2006
Jun;83(6):1289-96. PMID:
16762939
302
Miura K, Greenland P, Stamler J, Liu K, Daviglus ML, Nakagawa H.
Relation of Vegetable, Fruit, and Meat Intake to 7-Year Blood
Pressure Change in Middle-aged Men: The Chicago Western Electric
Study. Am J Epidemiol. 2004 Mar 15;159(6):572-80. PMID:
15003961
303
Alonso A, de la Fuente C, Martin-Arnau AM, de Irala J, Martinez
JA, Martinez-Gonzalez MA. Fruit and vegetable consumption is
inversely associated with blood pressure in a Mediterranean
population with a high vegetable-fat intake: the Seguimiento
Universidad de Navarra (SUN) Study. Br J Nutr. 2004 Aug;92(2):311-9.
PMID:
15333163
304
Beilin LJ, Burke V. Vegetarian diet components, protein and
blood pressure: which nutrients are important? Clin Exp Pharmacol
Physiol. 1995 Mar;22(3):195-8. Review. PMID:
7554413
305
Scheer FA, Van Montfrans GA, Van Someren EJ, Mairuhu G, Buijs RM.
Daily Nighttime Melatonin Reduces Blood Pressure in Male
Patients With Essential Hypertension. Hypertension. 2004 Jan 19
[Epub ahead of print] PMID:
14732734
306
Iseki K, Iseki C, Itoh K, Sanefuji M, Uezono K, Ikemiya Y,
Fukiyama K, Kawasaki T. Estimated protein intake and blood
pressure in a screened cohort in Okinawa, Japan. Hypertens Res. 2003
Apr;26(4):289-94. PMID:
12733696
307
Burke V, Hodgson JM, Beilin LJ, Giangiulioi N, Rogers P, Puddey
IB. Dietary protein and soluble fiber reduce ambulatory blood
pressure in treated hypertensives. Hypertension. 2001
Oct;38(4):821-6. PMID:
11641293
308
Effects of Protein, Monounsaturated Fat, and Carbohydrate Intake on
Blood Pressure and Serum Lipids: Results of the OmniHeart Randomized
Trial. JAMA. 2005 Nov 16;294(19):2455-2464. PMID:
16287956
309
http://www.ajcn.org/cgi/content/abstract/80/4/1012
310
Moderate Consumption of Olive Oil by Healthy European Men Reduces
Systolic Blood Pressure in Non-Mediterranean Participants. J Nutr.
2007 Jan;137(1):84-87. PMID:
17182805
311
Folic acid supplementation for 3 wk reduces pulse pressure and large
artery stiffness independent of MTHFR genotype. Am J Clin Nutr. 2005
Jul;82(1):26-31. PMID:
16002796
312
Low-fat dairy consumption and reduced risk of hypertension: the
Seguimiento Universidad de Navarra (SUN) cohort. Am J Clin Nutr.
2005 Nov;82(5):972-9. PMID:
16280427
313
Low-fat dairy consumption and reduced risk of hypertension: the
Seguimiento Universidad de Navarra (SUN) cohort. Am J Clin Nutr.
2005 Nov;82(5):972-9. PMID:
16280427
314
Short Sleep Duration as a Risk Factor for Hypertension. Analyses of
the First National Health and Nutrition Examination Survey.
Hypertension. 2006 Apr 3; PMID:
16585410
316
Kim YI, Role of Folate in Colon Cancer Development and
Progression. J. Nutr. 133:3731S-3739S, November 2003
318
Forman JP, Rimm EB, Stampfer MJ, Curhan GC. Folate intake and
the risk of incident hypertension among US women. JAMA. 2005 Jan
19;293(3):320-9. PMID:
15657325
319
Dose-dependent effects of folic acid on blood concentrations of
homocysteine: a meta-analysis of the randomized trials. Am J Clin
Nutr. 2005 Oct;82(4):806-812. PMID:
16210710
320
Clarke R, Grimley Evans J, Schneede J, Nexo E, Bates C, Fletcher
A, Prentice A, Johnston C, Ueland PM, Refsum H, Sherliker P, Birks
J, Whitlock G, Breeze E, Scott JM. Vitamin B12 and folate
deficiency in later life. Age Ageing. 2004 Jan;33(1):34-41. PMID:
14695861
321
Harwood RH, Sahota O, Gaynor K, Masud T, Hosking DJ. A
randomised, controlled comparison of different calcium and vitamin D
supplementation regimens in elderly women after hip fracture: The
Nottingham Neck of Femur (NONOF) Study. Age Ageing. 2004
Jan;33(1):45-51. PMID:
14695863
322
The case against ergocalciferol (vitamin D2) as a vitamin
supplement. Am J Clin Nutr. 2006 Oct;84(4):694-7. PMID:
17023693
323
Munger KL, Zhang SM, O'Reilly E, Hernan MA, Olek MJ, Willett WC,
Ascherio A. Vitamin D intake and incidence of multiple
sclerosis. Neurology. 2004 Jan 13; 62(1): 60-5. PMID:
14718698
324
Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis.
JAMA. 2006 Dec 20;296(23):2832-8. PMID:
17179460
325
Holick MF. Vitamin D: importance in the prevention of
cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin
Nutr. 2004 Mar;79(3):362-71. PMID: 14985208
326
http://www.ajcn.org/cgi/content/full/69/5/842
327
Grant WB. Ecologic studies of solar UV-B radiation and cancer
mortality rates. Recent Results Cancer Res. 2003;164:371-7. Review.
PMID:
12899536
329
The Role of Vitamin D in Cancer Prevention. Am J Public Health. 2005
Dec 27; [Epub ahead of print] PMID:
16380576
331
Science News, 2006-11-11, p312
333
Zandi PP, Anthony JC, Khachaturian AS, Stone SV, Gustafson D,
Tschanz JT, Norton MC, Welsh-Bohmer KA, Breitner JC. Reduced
risk of Alzheimer disease in users of antioxidant vitamin
supplements: the cache county study. Arch Neurol. 2004 Jan; 61(1):
82-8. PMID:
14732624
334
Eidelman RS, Hollar D, Hebert PR, Lamas GA, Hennekens CH.
Randomized trials of vitamin E in the treatment and prevention of
cardiovascular disease. Arch Intern Med. 2004 Jul 26;164(14):1552-6.
PMID:
15277288
335
Miller ER 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel
LJ, Guallar E. Meta-analysis: high-dosage vitamin E
supplementation may increase all-cause mortality. Ann Intern Med.
2005 Jan 4;142(1):37-46. Epub 2004 Nov 10. PMID:
15537682
336
Ames BN. Review Article: Delaying the Mitochondrial Decay of Aging-a
Metabolic Tune-up. Alzheimer Dis Assoc Disord. 2003 Apr-Jun;17(2
Suppl):S54-7. No abstract available. PMID:
12813210
337
Troost FJ, Saris WH, Haenen GR, Bast A, Brummer RJ. New
method to study oxidative damage and antioxidants in the human small
bowel: effects of iron application. Am J Physiol Gastrointest Liver
Physiol. 2003 Aug;285(2):G354-9. Epub 2003 Apr 30. PMID:
12724133
339
Aureli T, Di Cocco ME, Capuani G, Ricciolini R, Manetti C,
Miccheli A, Conti F. Effect of long-term feeding with
acetyl-L-carnitine on the age-related changes in rat brain lipid
composition: a study by 31P NMR spectroscopy. Neurochem Res. 2000
Mar;25(3):395-9. PMID:
10761985
340
Shoba G, Joy D, Joseph T, Majeed M, Rajendran R, Srinivas PS.
Influence of piperine on the pharmacokinetics of curcumin in
animals and human volunteers. Planta Med. 1998 May;64(4):353-6.
PMID:
9619120
341
Curry Consumption and Cognitive Function
in the Elderly American Journal of Epidemiology Advance
Access published on July 26, 2006 Am. J. Epidemiol. 2006 164:
898-906 PMID:
16870699
343
Dietary Intake of Calcium in Relation to Mortality From
Cardiovascular Disease. The JACC Study. Stroke. 2005 Dec 8; [Epub
ahead of print] PMID:
16339476
344
Lopez-Ridaura R, Willett WC, Rimm EB, Liu S, Stampfer MJ, Manson
JE, Hu FB. Magnesium Intake and Risk of Type 2 Diabetes in Men
and Women. Diabetes Care. 2004 Jan;27(1):134-140. PMID: 14693979
346
Larsson SC, Bergkvist L, Wolk A. Magnesium intake in relation
to risk of colorectal cancer in women. JAMA. 2005 Jan 5;293(1):86-9.
PMID:
15632340
347
Magnesium Intake and Reduced Risk of Colon Cancer in a Prospective
Study of Women. Am J Epidemiol. 2005 Nov 30; [Epub ahead of print]
PMID:
16319289
349
Oral magnesium supplementation in asthmatic children: a double-blind
randomized placebo-controlled trial. Eur J Clin Nutr. 2007
Jan;61(1):54-60. Epub 2006 Jun 21. PMID:
16788707
350
Klein EA. Selenium: Epidemiology and Basic Science. J Urol.
2004 Feb;171(2):S50-S53. PMID:
14713754
351
Hammes HP, Du X, Edelstein D, Taguchi T, Matsumura T, Ju Q, Lin
J, Bierhaus A, Nawroth P, Hannak D, Neumaier M, Bergfeld R, Giardino
I, Brownlee M. Benfotiamine blocks three major pathways of
hyperglycemic damage and prevents experimental diabetic retinopathy.
Nat Med. 2003 Mar;9(3):294-9. Epub 2003 Feb 18. PMID:
12592403
352
Babaei-Jadidi R, Karachalias N, Ahmed N, Battah S, Thornalley PJ.
Prevention of incipient diabetic nephropathy by high-dose
thiamine and benfotiamine. Diabetes. 2003 Aug;52(8):2110-20. PMID:
12882930
353
Weindruch R, Walford RL, Fligiel S, Guthrie D. The
retardation of aging in mice by dietary restriction: longevity,
cancer, immunity and lifetime energy intake. J Nutr. 1986
Apr;116(4):641-54. PMID:
3958810
354
Tucker KL, Hannan MT, Qiao N, Jacques PF, Selhub J, Cupples LA,
Kiel DP. Low plasma vitamin B12 is associated with lower BMD:
the Framingham Osteoporosis Study. J Bone Miner Res. 2005
Jan;20(1):152-8. Epub 2004 Oct 25. PMID:
15619681
355
Methylmalonic acid and cognitive function in the Medical Research
Council Cognitive Function and Ageing Study. Am J Clin Nutr. 2006
PMID:
17158424
356
Feskanich D, Willett WC, Stampfer MJ, Colditz GA. Milk,
dietary calcium, and bone fractures in women: a 12-year prospective
study. Am J Public Health. 1997 Jun;87(6):992-7. PMID:
9224182
357
Dietary intake of antioxidants and risk of age-related macular
degeneration. JAMA. 2005 Dec 28;294(24):3101-7. PMID:
16380590
358
Hu FB, Willett WC. Optimal diets for prevention of coronary
heart disease. JAMA. 2002 Nov 27;288(20):2569-78. Review. PMID:
12444864
359
Sacks FM, Katan M. Randomized clinical trials on the effects
of dietary fat and carbohydrate on plasma lipoproteins and
cardiovascular disease. Am J Med. 2002 Dec 30;113 Suppl 9B:13S-24S.
Review. PMID:
12566134
360
Hung T, Sievenpiper JL, Marchie A, Kendall CW, Jenkins DJ.
Fat versus carbohydrate in insulin resistance, obesity, diabetes and
cardiovascular disease. Curr Opin Clin Nutr Metab Care. 2003
Mar;6(2):165-76. PMID:
12589186
362
Smith AP. Breakfast cereal consumption and subjective reports
of health. Int J Food Sci Nutr. 1999 Nov;50(6):445-9. PMID:
10719585
363
Smith AP, Clark R, Gallagher J. Breakfast cereal and
caffeinated coffee: effects on working memory, attention, mood, and
cardiovascular function. Physiol Behav. 1999 Aug 1;67(1):9-17. PMID:
10463623
365
Farshchi HR, Taylor MA, Macdonald IA. Deleterious effects of
omitting breakfast on insulin sensitivity and fasting lipid profiles
in healthy lean women. Am J Clin Nutr. 2005 Feb;81(2):388-96. PMID:
15699226
366
Appel LJ. The effects of protein intake on blood pressure and
cardiovascular disease. Curr Opin Lipidol. 2003 Feb;14(1):55-9.
PMID:
12544662
367
Powers KM, Smith-Weller T, Franklin GM, Longstreth WT Jr, Swanson
PD, Checkoway H. Parkinson's disease risks associated with
dietary iron, manganese, and other nutrient intakes. Neurology. 2003
Jun 10;60(11):1761-1766. PMID:
12796527
369
Yokoo EM, Valente JG, Grattan L, Schmidt SL, Platt I, Silbergeld
EK.Low level methylmercury exposure affects neuropsychological
function in adults. Environ Health. 2003 Jun 4;2(1):8. Epub 2003 Jun
04. PMID: 12844364 free
full text
370
Guillen MD, Sopelana P, Partearroyo MA. Polycyclic aromatic
hydrocarbons in liquid smoke flavorings obtained from different
types of wood. Effect of storage in polyethylene flasks on their
concentrations. J Agric Food Chem. 2000 Oct;48(10):5083-7. PMID:
11052782
373
Gorell JM, Peterson EL, Rybicki BA, Johnson CC. Multiple risk
factors for Parkinson's disease. J Neurol Sci. 2004 Feb
15;217(2):169-74. PMID:
14706220
374
Miu AC, Andreescu CE, Vasiu R, Olteanu AI. A behavioral and
histological study of the effects of long-term exposure of adult
rats to aluminum. Int J Neurosci. 2003 Sep;113(9):1197-211. PMID:
12959739
375
Wong MH, Fung KF, Carr HP. Aluminium and fluoride contents of
tea, with emphasis on brick tea and their health implications.
Toxicol Lett. 2003 Jan 31;137(1-2):111-20. Review. PMID:
12505437
377
Soy diet worsens heart disease in mice. J Clin Invest. 2006
Jan;116(1):209-16. PMID:
16395406
378
Miller ER 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel
LJ, Guallar E. Meta-analysis: high-dosage vitamin E
supplementation may increase all-cause mortality. Ann Intern Med.
2005 Jan 4;142(1):37-46. Epub 2004 Nov 10. PMID:
15537682
381
Inflammatory markers and particulate air pollution: characterizing
the pathway to disease. Int J Epidemiol. 2006 Jul 14; PMID:
16844771
382
Dietary Copper and High Saturated and trans Fat Intakes Associated
With Cognitive Decline. Arch Neurol. 2006 Aug;63(8):1085-1088. PMID:
16908733
383
Zinc, copper, and magnesium and risks for all-cause, cancer, and
cardiovascular mortality. Epidemiology. 2006 May;17(3):308-14. PMID:
16570028
386
Tsai CJ, Leitzmann MF, Willett WC, Giovannucci EL. Dietary
Protein and the Risk of Cholecystectomy in a Cohort of US Women: The
Nurses' Health Study. Am J Epidemiol. 2004 Jul 1;160(1):11-8. PMID:
15229112
387
The relation between dietary protein, calcium and bone health in
women: results from the EPIC-Potsdam cohort. Ann Nutr Metab. 2005
Sep-Oct;49(5):312-8. Epub 2005 Aug 4. PMID:
16088096
388
Dietary protein and risk of ischemic heart disease in women. Am J
Clin Nutr. 1999 Aug;70(2):221-7. PMID:
10426698
389
Methionine-deficient diet extends mouse lifespan, slows immune and
lens aging, alters glucose, T4, IGF-I and insulin levels, and
increases hepatocyte MIF levels and stress resistance. Aging Cell.
2005 Jun;4(3):119-25. PMID:
15924568
390
Nutritional control of aging. Exp Gerontol. 2003
Jan-Feb;38(1-2):47-52. PMID:
12543260
391
Low methionine ingestion by rats extends life span. J Nutr. 1993
Feb;123(2):269-74. PMID:
8429371
392
Methionine restriction decreases visceral fat mass and preserves
insulin action in aging male Fischer 344 rats independent of energy
restriction. Aging Cell. 2006 Jun 26; [Epub ahead of print] PMID:
16800846
393
Methionine restriction inhibits colon carcinogenesis. Nutr Cancer.
2006;54(2):202-8. PMID:
16898864
394
Caloric restriction and aging: controversial issues. J Gerontol A
Biol Sci Med Sci. 2006 Jan;61(1):14-9. Review. PMID: 16456190
397
Colas, but not other carbonated beverages, are associated with low
bone mineral density in older women: The Framingham Osteoporosis
Study. Am J Clin Nutr. 2006 Oct;84(4):936-42. PMID:
17023723
398
Soder PO, Soder B, Nowak J, Jogestrand T. Early carotid
atherosclerosis in subjects with periodontal diseases. Stroke. 2005
Jun;36(6):1195-200. Epub 2005 May 5. PMID:
15879347
399
Dental and Periodontal Status and Risk for Progression of Carotid
Atherosclerosis. The Inflammation and Carotid Artery Risk for
Atherosclerosis Study Dental Substudy. Stroke. 2006 Aug 3; PMID:
16888276
401
Lipoprotein particle profiles mark familial and sporadic human
longevity. PLoS Med. 2006 Dec;3(12):e495. PMID:
17194192
402
Bayman P, Baker JL, Mahoney NE. Aspergillus on tree nuts:
incidence and associations. Mycopathologia. 2002;155(3):161-9. PMID:
12617503